
Adderall Suicide
Case #231

A 21-year-old man presented to a psychiatric nurse practitioner in 2013.
The chief complaint was listed as “poor concentration, poor focus, distractible, depressed, good sleep, mind races”.
The psychiatric history was noteworthy for ADHD diagnosis in elementary school and use of both Ritalin and Strattera at several points.
She also noted a psychiatric hospitalization in 2008 when he was 16, after his pediatrician became aware that he was suicidal.
The patient reported occasional cannabis use and binge drinking.
Both suicidal and homicidal ideation were denied.
She prescribed Concerta 36mg qday.
At a follow-up appointment, he was still reporting inattentiveness with a poor attention span.
Concerta was switched to Adderall XR 20mg qday.
At the next few appointments, he reported feeling much better.
However, at his final appointment several months later, he reported having problems completing tasks and felt he was easily distracted.
Adderall was increased to 30mg qday.
He continued to deny suicidal ideation.
The patient died by suicide 6 weeks later, in March 2014.
Become a better doctor.
Join thousands of doctors who are improving their practice by reviewing cases.
His family sued the NP and her employer.
The primary criticism was that the NP did not obtain previous records from 3 different sources, which included information that may have altered her decision to diagnose him with ADHD and start Adderall.
The first hospitalization in 2008 (age 16) was due to the fact that he set up a rope and ladder in the backyard and stated that he was going to kill himself. His family felt that Strattera (started several months prior to this suicidal gesture) was causing him to become more depressed. It was discontinued.
Two years before his death, the patient was being seen by an outpatient psychiatrist, Dr. H. She diagnosed him with bipolar disorder, with rapid cycling between depression and mania. ADHD was felt to be a historical diagnosis and Adderall was discontinued.
A second hospitalization occurred in 2012 when he was 20-years-old, just a few months before he started seeing the NP. It does not appear the NP ever knew about this hospitalization. This hospitalization was triggered by a series of events including putting a gun in his mouth in front of his mother while threatening suicide, multiple arrests in a short period of time, hypersexual behavior, physical fights with his father, and breaking windows in a fit of rage. He was noted to have constant suicidal ideation, and the inpatient team agreed with the diagnosis of bipolar disorder, and did not list ADHD as a diagnosis.
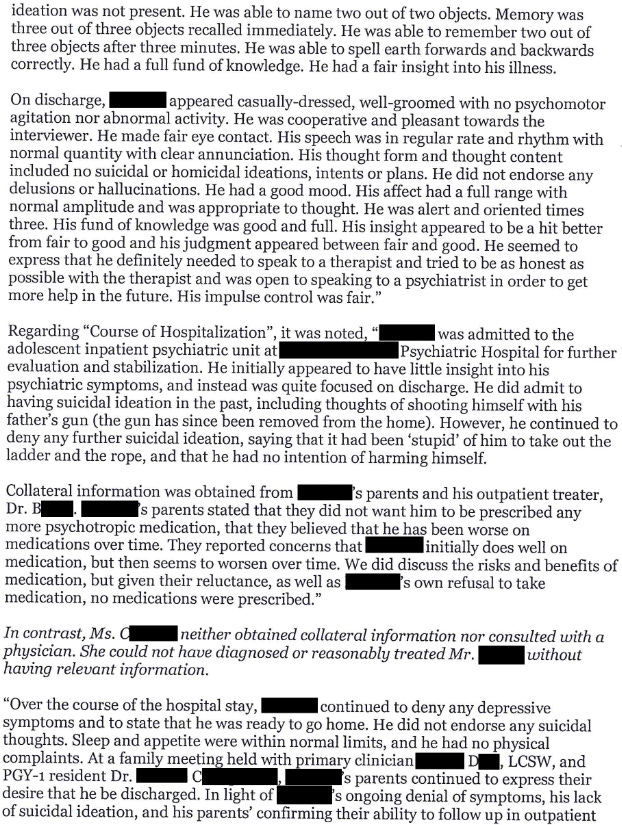
The expert witness opinion is shown here:













The defense filed a motion to dismiss the lawsuit because the expert did not clarify their training.
The motion was granted and the lawsuit was dismissed.
The lawsuit was refiled with clarification of the expert’s credentials.
It appears it was subsequently settled.
Paying subscribers get a new case every week and access to the entire archive.
MedMalReviewer Analysis:
I don’t understand why the patient stopped seeing the board-certified psychiatrist and switched to a nurse practitioner. All of the criticisms against the NP would have been avoided by remaining under the care of the same physician who had a good understanding of his history. Its not clear if the psychiatrist moved or shut down her practice, or if there was a breakdown in the patient-doctor relationship. Regardless of the reason, this case is an excellent example of how discontinuity of care is dangerous.
It seems that the NP was only aware of the 2008 hospitalization when the patient was 16-years-old. I’m not convinced that obtaining these records would have altered her decision-making when she saw him 5 years later. Additionally, it’s hard to fault her for not obtaining records from the 2012 hospitalization if she wasn’t told about it.
The causative role of Adderall in the patient’s suicide is up for debate. He denied suicidal thoughts at each visit, even after re-starting Adderall. He had been on even higher doses of Adderall previously. The patient certainly had a history of extremely concerning suicidal behavior, but it doesn’t appear that any of these happened in the months preceding his death while under the NP’s care.
The expert takes the criticism a bit too far in my opinion. They claim the NP should have contacted the 21-year-old patient’s pediatrician. They claim that a suicide assessment can’t be completed without obtaining all of a patient’s past records. The NP’s care certainly could have been better at multiple points, but I’m not sure that any of the alleged shortcomings caused the patient’s suicide, nor would fixing them have prevented his death.
I’ve published other psych-related cases, including this case that deals with questionable prescriptions shortly before a suicide.
This patient was a wealthy investment banker who was started on testosterone while in a psych facility.
A visitor smuggled chloroquine to him, which he used to end his life while in the psych hospital.

Why did he see a NP as opposed to a board-certified psychiatrist? Perhaps to obtain Adderall?
I had to mind my biases on this one because, while not a 100% accurate generalization, psych NPs being too casual with stimulants for vague complaints of "can't focus" is almost a meme among psychiatrists.
But having said that, I think this lawsuit was probably an effort to monetize a tragedy. Some sloppy work, but not so sloppy I would say it caused this patient's suicide, and if a patient (an adult patient, no less) only volunteers a history of ADHD and withholds everything else, I'm not sure how an NP would be expected to even know that there is relevant collateral available, much less how to get it. It's easy for me to say from my couch that I would do a more thorough inspection for ADHD or demand prior records verifying the diagnosis, but saying that not doing so led to this patient killing themselves is a stretch.
As it stands, the expert's opinion here just seems to read as a grab-bag of pedantic criticism, rather than presenting an actual theory for what the NP specifically did that led to the patient's suicide.
I'm honestly surprised that psychiatry is one of the least-sued specialties because if providers can be sued for failing to read their patients' minds, I would think nearly every case of suicide could be converted to at least a settlement extraction if the surviving family can find an attorney with a pulse.