


Atraumatic Ankle Pain [Pseudogout vs Septic Joint]
Case #245

A 50-year-old man presented to the ED with atraumatic pain in his left ankle.
It was noted to be swollen, erythematous, and painful with movement.
X-rays were negative.
The patient was admitted by the hospitalist (Dr. G).
A rheumatologist (Dr. V) saw the patient and ordered an ankle arthrocentesis.
The crystal result were suggestive of pseudogout.
The patient was discharged and given the rheumatologist’s office phone number for follow-up.
Improve your practice by reviewing malpractice cases.
Paying subscribers get a new case every week and access to the entire archive.
Later in the day after the patient was discharged, the synovial fluid cultures came back positive for staphylococcus aureus.
This was considered a critical result, so the lab tech was required to notify a physician.
Hospital policy dictated that when a discharged patient had a critical result, the lab techs should first attempt to contact the primary care physician.
The lab tech followed the protocol, and called the patient’s primary care office.
The primary care office and the hospital were in different healthcare systems and did not have direct access to each other’s records.
The on-call physician (Dr. T) for the primary care group took the call. He was not the patient’s PCP.
A miscommunication occurred, and Dr. T believed the patient was still admitted. He believed that the inpatient team would address the critical result.
An automatic message was generated to the discharging hospitalist’s inbox, but no call was made to her.
The patient followed up with his primary care doctor (Dr. S) several times.
Dr. S did not have direct access to the hospital records and his colleague Dr. T never advised him of the positive culture result.
The following month, the patient presented to the hospital with fever, malaise, and neck pain.
He was found to have a cervical epidural abscess and staph aureus bacteremia.
His ankle was still swollen and causing pain.
The patient was treated and survived, but has limited mobility due to lingering pain and dysfunction of his left ankle.
The patient sued the rheumatologist, the primary care doctor who answered the call from the lab, and the patient’s primary care doctor.
They sued the primary care physician group itself and the hospital.
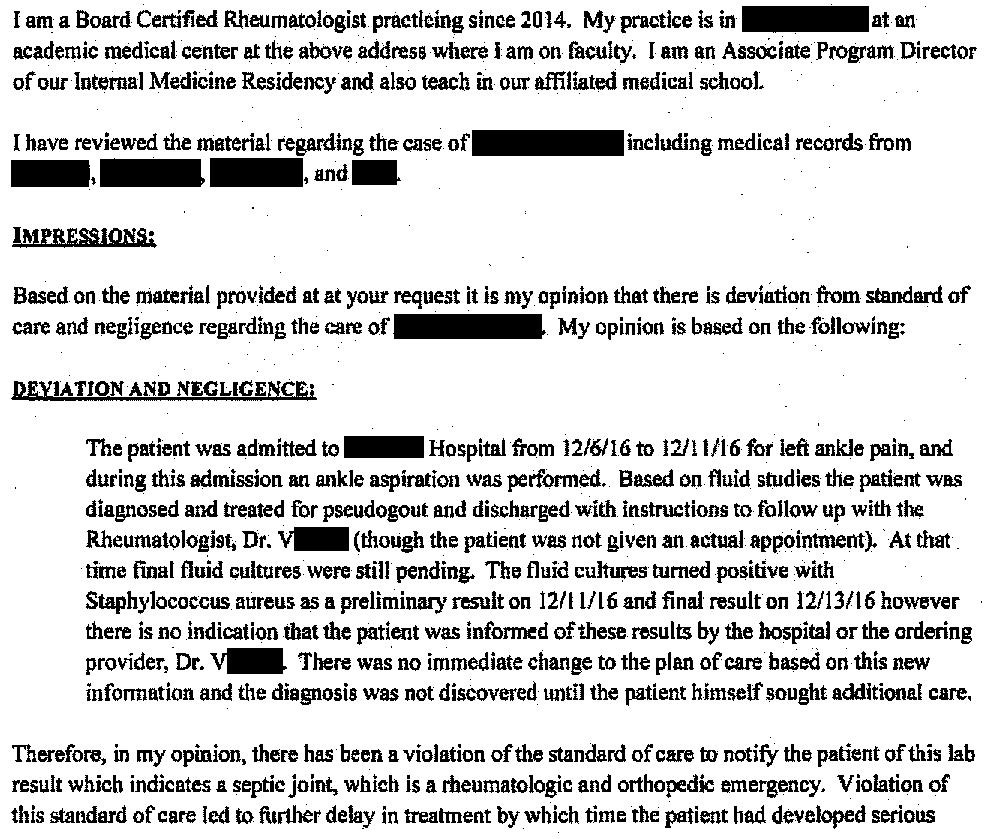
The plaintiff’s rheumatology expert opinion is shown here:

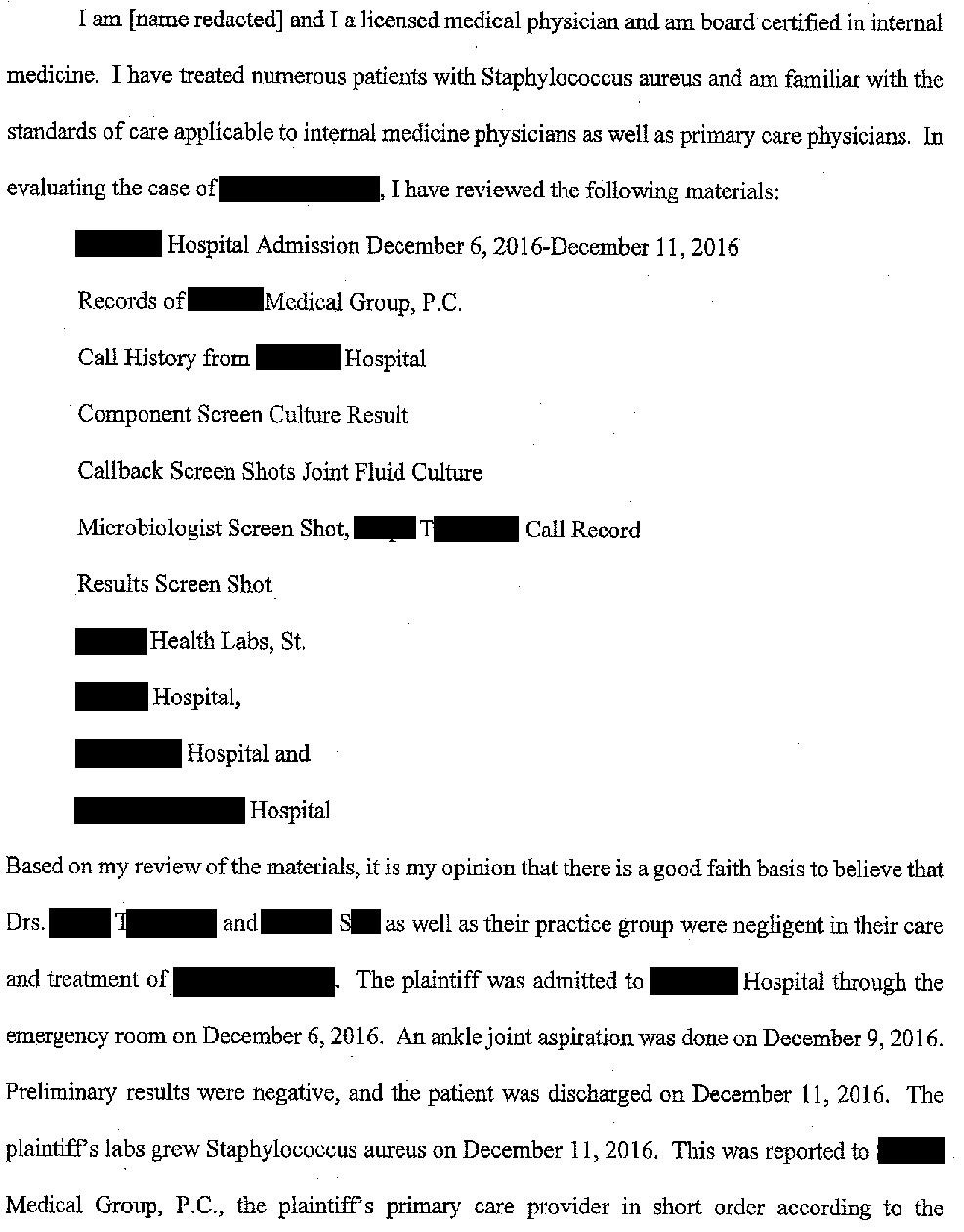
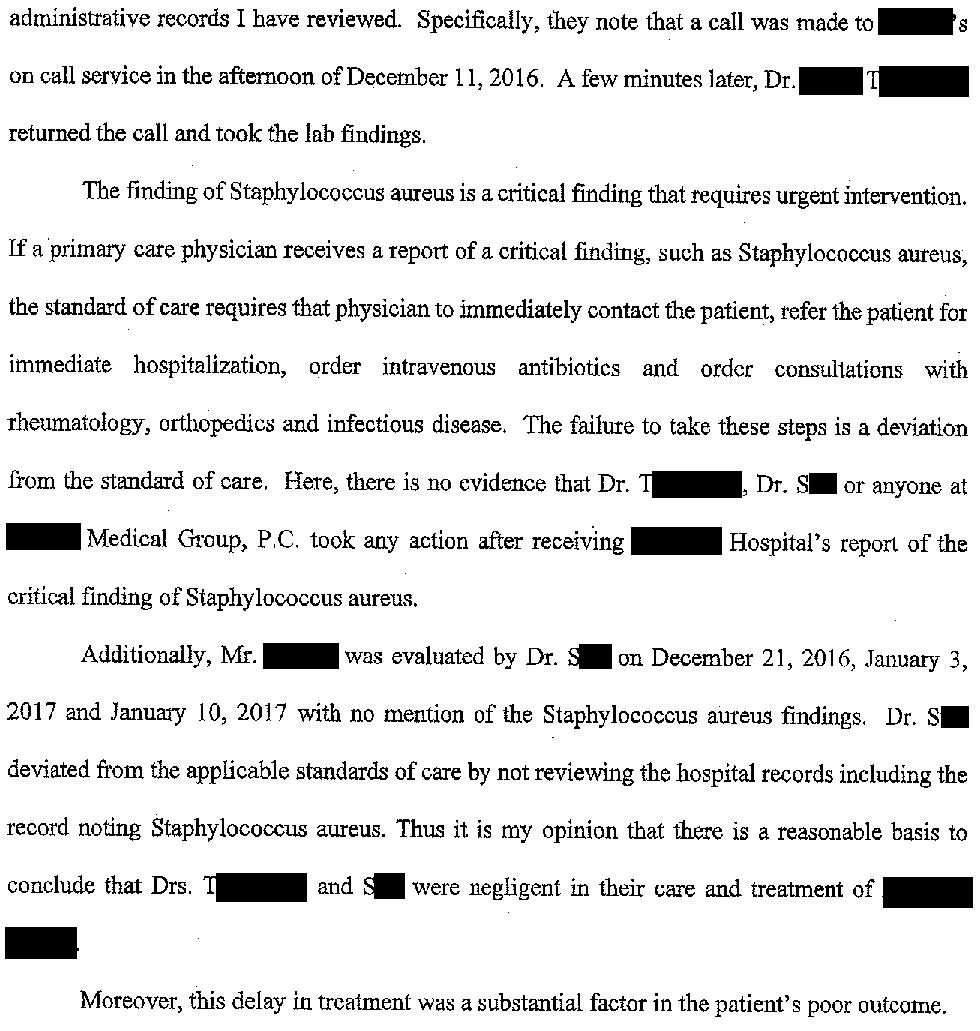
The plaintiff’s primary care expert opinion is shown here:
Become a better doctor.
Learn from other doctor’s mistakes to reduce the likelihood that you’ll get sued.
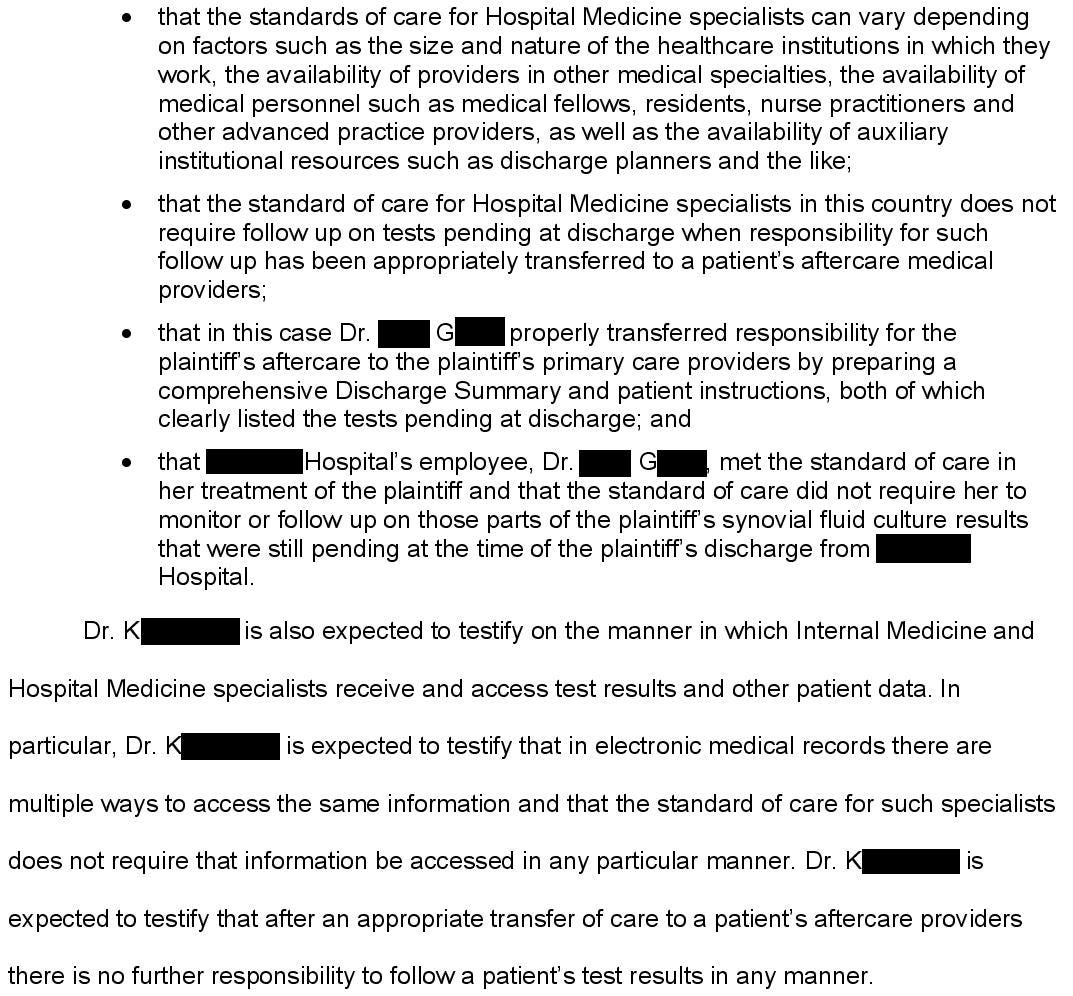
The hospital’s defense attorney hired a hospitalist expert to defend the care of their employee, the discharging hospitalist (Dr. G).

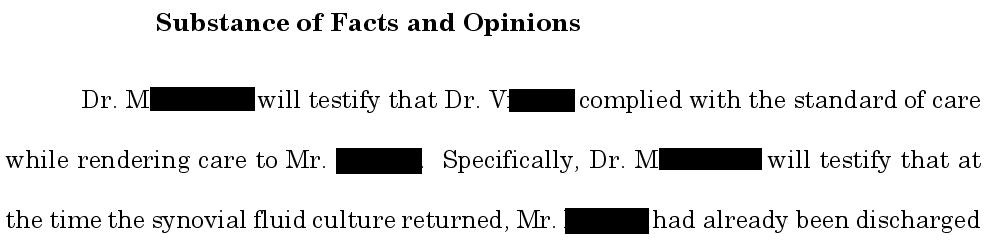
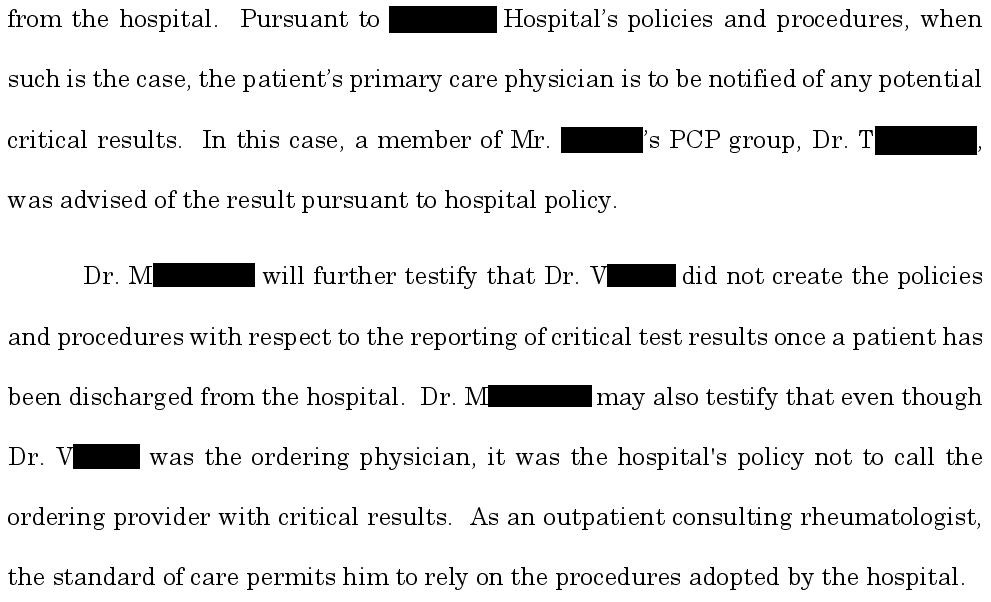
The rheumatologist’s defense attorney hired a rheumatology expert:
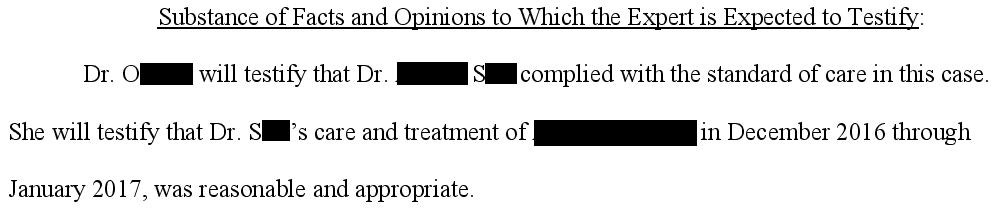
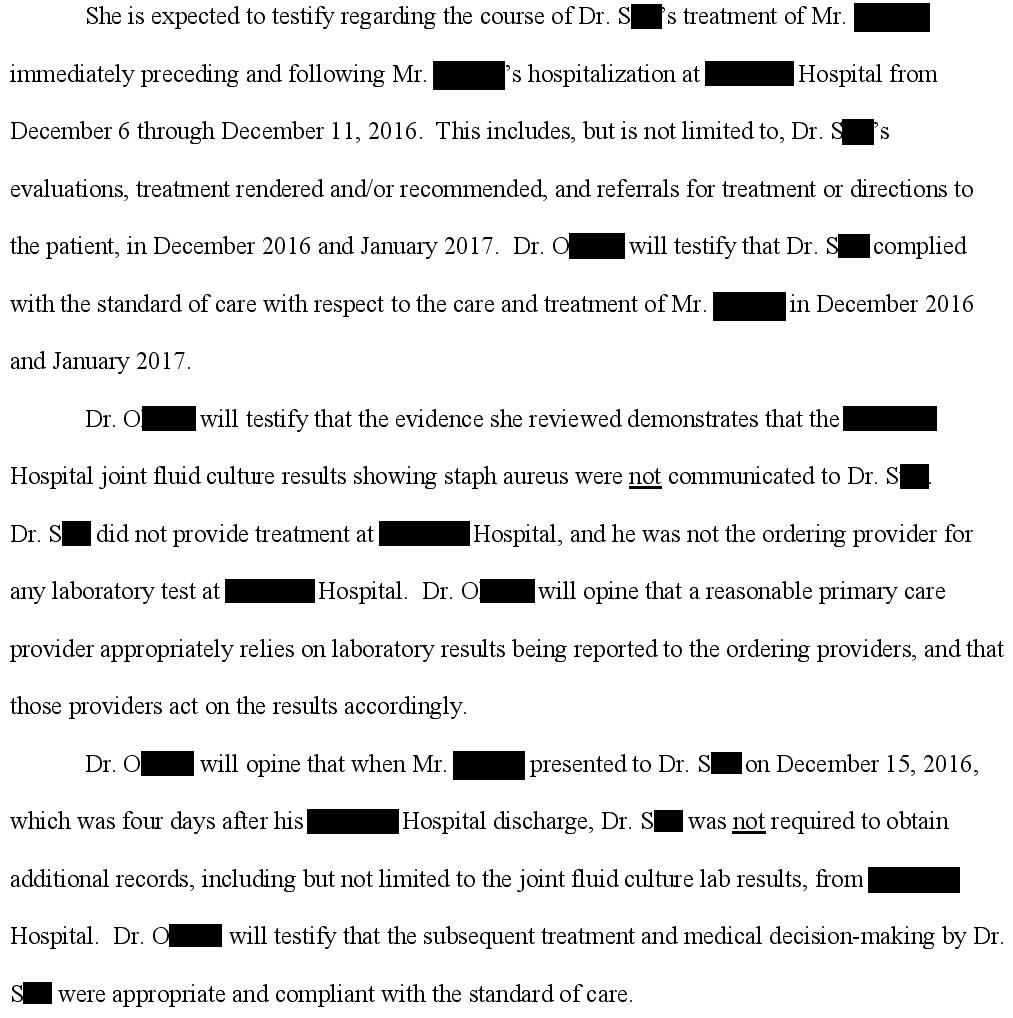
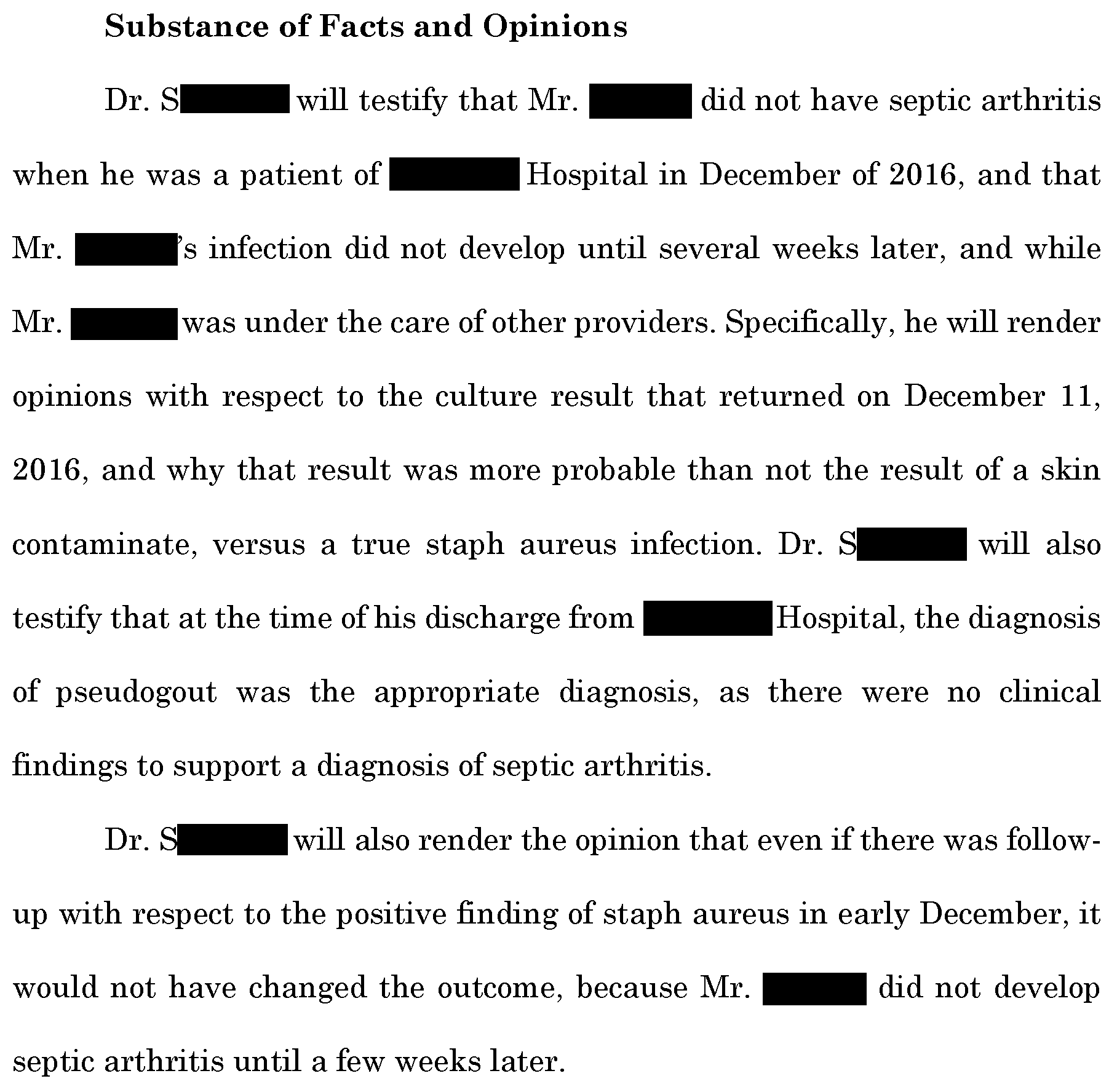
The defense hired a primary care expert to defend Dr. S, the patient’s primary care doctor who saw the patient after discharge but did not realize there were positive cultures results.
Finally, the defense hired an infectious disease expert who suggested that the positive culture result was actually contaminant.
The plaintiff hired a financial expert who assessed the patient’s lost income.

They offered to settle the case for $6,000,000.

The lawsuit reached a confidential settlement before trial.
MedMalReviewer Analysis:
This is a challenging case because the patient suffered real harm that was absolutely preventable, but each individual doctor has a reasonable defense. Part of me wants to criticize the fact that all of the doctors did the bare minimum, nobody took ownership to follow-up on pending results, and they all simply passed the buck to someone else. But overall I think this was more of a systems failure. The fact that the critical result was called to the patient’s PCP office instead of the ordering or discharging doctor could be criticized. The fact that we don’t have a universal electronic medical record that can be accessed by doctors in different practice groups certainly played into this as well.
The easiest physician to criticize here is Dr. T, who took the call from the lab and never did anything about it. However, I wonder if there is some critical context that helps explain his inaction. I suspect there was a miscommunication and he believed that the patient was still admitted, in which case it’s reasonable to believe that the inpatient doctor would address this. I wouldn’t be surprised if he had gotten numerous calls before about culture results, most of which are contaminant. In a busy practice, the on-call doctor may take dozens of calls per day, and it’s easy to understand how a call might slip your mind if you have multiple issues all simultaneously competing for your attention.
Even after reading all the court documents, it’s not clear to me why the patient was admitted to the hospital. An ankle arthrocentesis should be an ED procedure, you don’t need to admit someone for a rheumatology consult to get an ankle tap. It’s also odd that they waited several days to tap the ankle.
I don’t find very many cases in which a rheumatologist was sued. I was hoping to find a nuanced rheumatology case that would be intellectually stimulating, so it was a bit disappointing that it was just a follow-up issue. But I think in a lot of ways this is emblematic of most malpractice cases. We’re pretty good at the actual medical decision-making. We’ve spent decades training to learn the pathophysiology. But so many malpractice cases don’t have anything to do with medical knowledge, they’re simply due to miscommunication, logistical challenges, poor handoffs, or systems issues. Those are the issues that you’re much more likely to get sued for (causing years of anxiety and burnout), but you really won’t get much education about them unless you make a consistent habit of reading malpractice cases.
The fact the patient was never informed of the positive culture result is the craziest part in my opinion.
I think this is a very interesting case of MISCOMMUNICATION that led to a big settlement despite the ankle tap being considered a contaminant.
I agree that Dr. T could have prevented this lawsuit perhaps if he had only COMMUNICATED with someone else. If I took this call as a provider oncall who did not know the patient, I would have just CALLED THE OFFICE and spoke with the PCPs office staff to inform them. I ALSO make it a habit to CALL the patient as well. If I was called from the hospital lab, I would ask them "is this patient still in the hospital?" If so I would call the floor and make sure the hospitalist was aware of the information. Since this patient had been discharged I would CALL THE PATIENT since cell phone numbers are in the hospital system and discussed it with them as well. Directly communicating with the patient helps prevent problems down the road including preventing lawsuits!
The above takes a matter of 5-10 minutes. I would do this SINCE I was called from a HOSPITAL LAB with a CRITICAL VALUE. In these cases, I ALWAYS make sure that someone else is aware of this. Even though we look at culture results all the time, I think there is more importance to this particular type of result.
The above all comes down to COMMON SENSE and TAKING CARE OF THE PATIENT. Attention to details especially when YOU the provider are involved in an unexpected clinical situation that may result in a bad outcome is of KEY IMPORTANCE. In fact, I just called the ER after my shift 2 days ago to follow up on a patient with early pregnancy who had a send out beta hCG with no follow up. Patient was out of town and came in for pelvic pain and positive hCG. So as an OBGYN who also does ER work, I made SURE that I communicated the results to the patient and there was follow up ASAP. Patients like this never have a good means of follow up. I made sure this patient knew the results and could be seen the following day. If this resulted in a ruptured ectopic with emergency surgery it's obvious what would happen when the request for records came around. It is hard to make sure patients get follow up even though we stress this in the ER when they are seen. LUCKILY, WE DO HAVE A SYSTEM IN PLACE FOR LAB FOLLOW UP IN THE ER TO HELP PREVENT THOSE IMPORTANT LAB RESULTS THAT MAY GET OVERLOOKED WITH NO COMMUNICATION TO ANOTHER PATIENT OR HEALTHCARE PROVIDER. WE SHOULD NEVER ASSUME THAT IT WILL BE TAKEN CARE OF BY SOMEONE ELSE PERHAPS SIMILAR TO THIS CASE.
Reviewing MedMal cases like this definitely help to prevent these problems in the future.