


Carotid Blowout Syndrome [Oncology]
Case #73

A 49-year-old man presented to a local ENT with chronic right ear pain.
Physical exam did not show any apparent cause, therefore a CT scan was ordered.
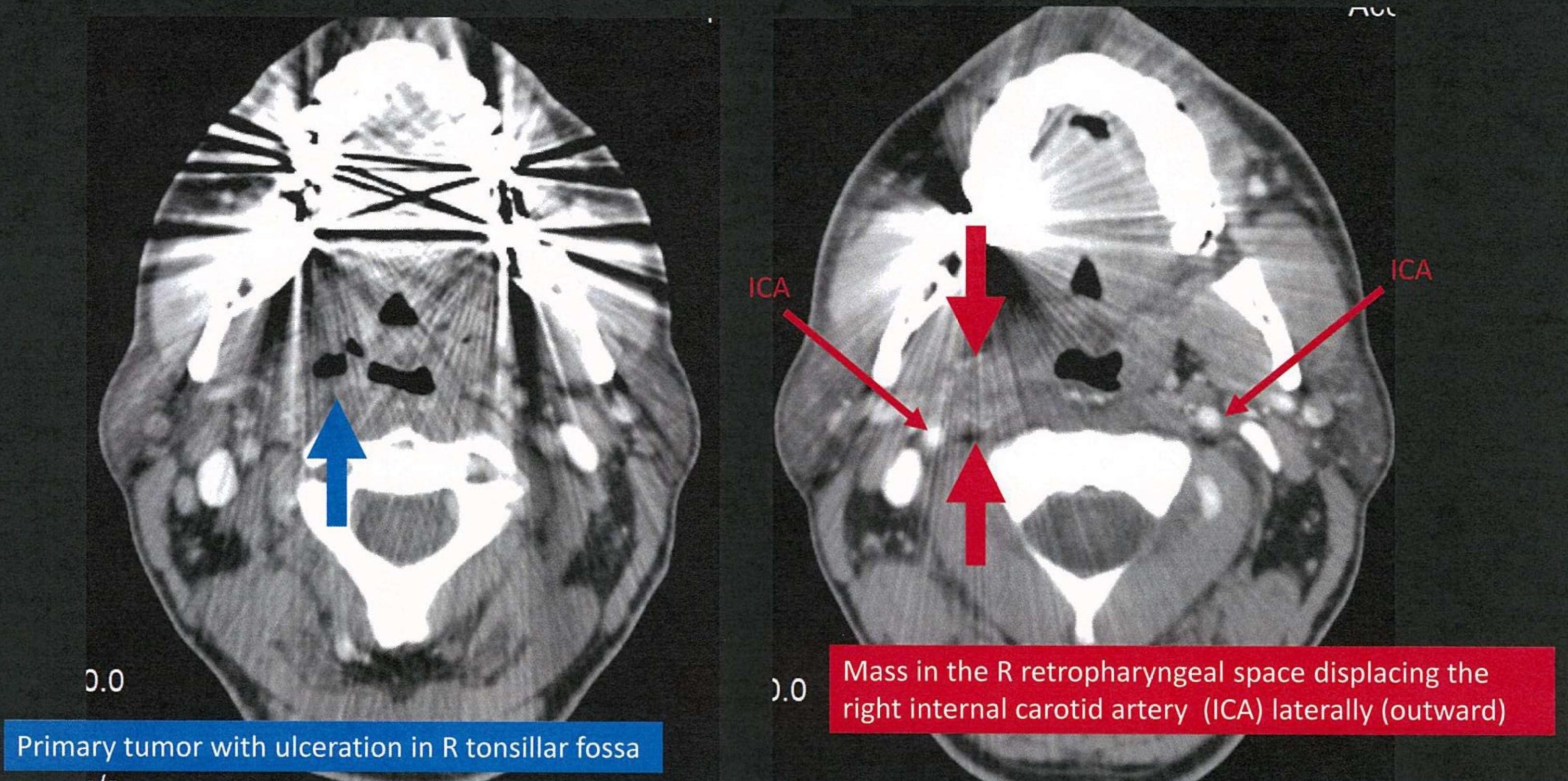
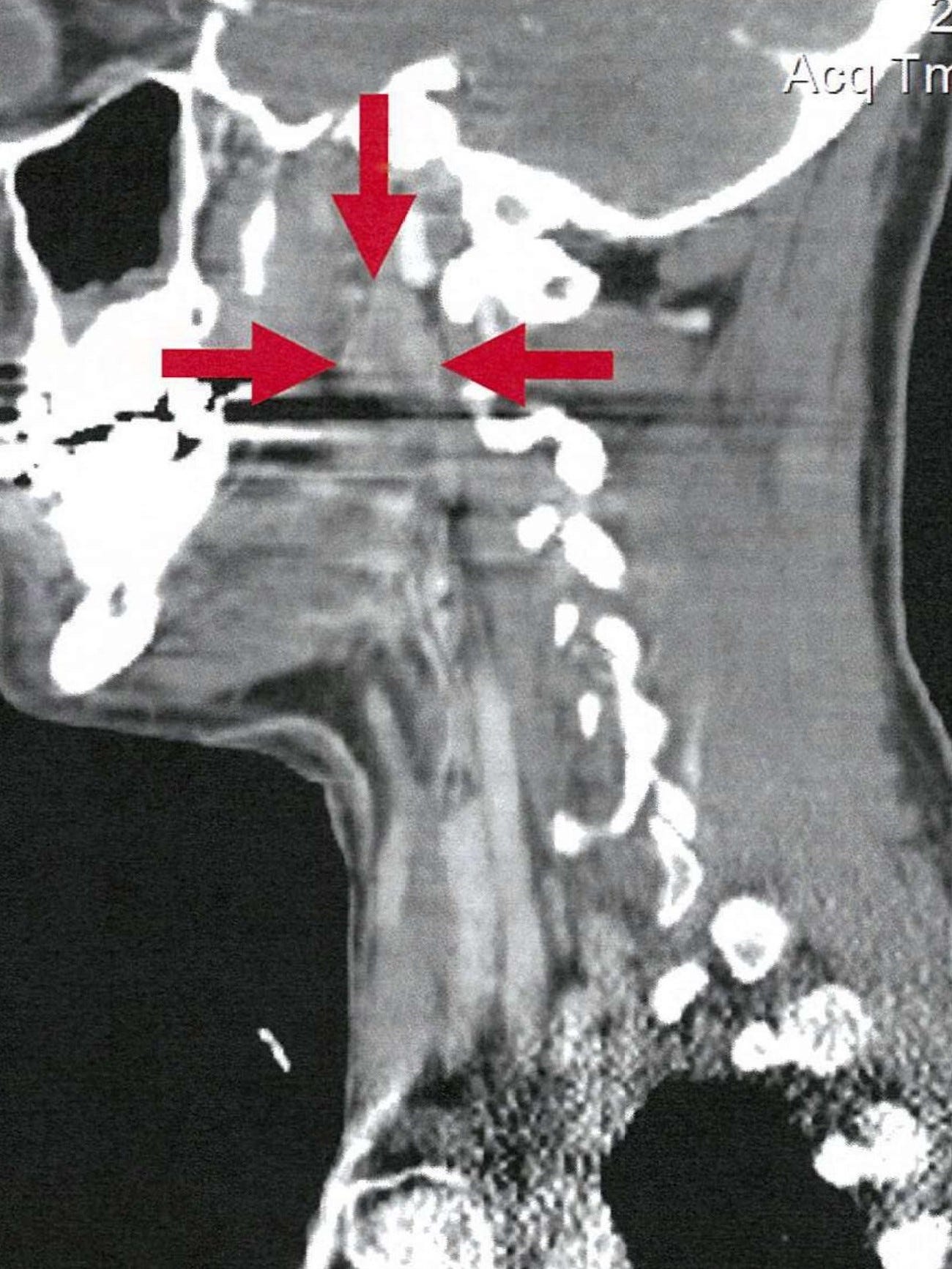
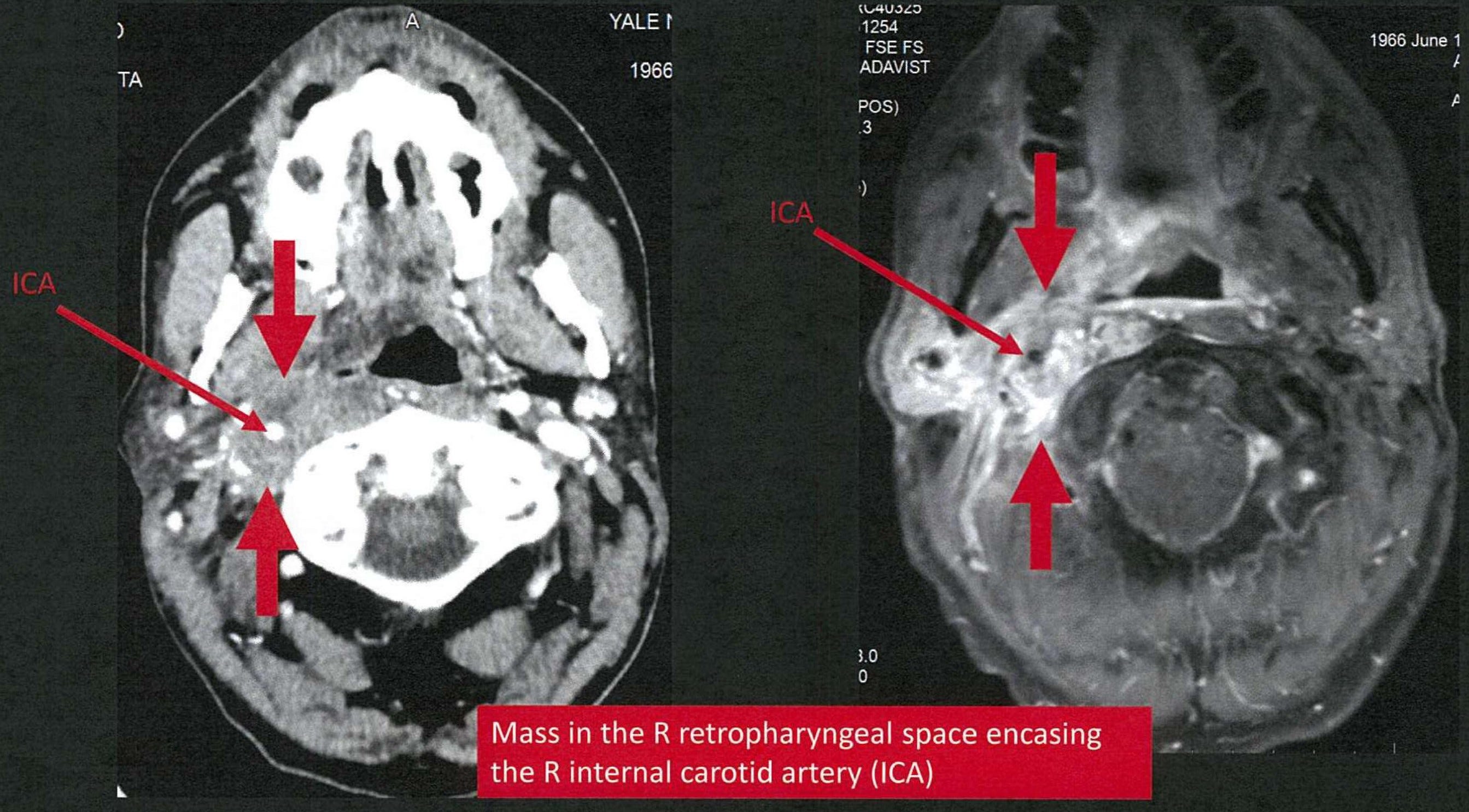
The CT revealed a 1.4cm mass in the right pharyngeal space and a 1.6cm lymph node in the right retropharyngeal/parapharyngeal carotid space.
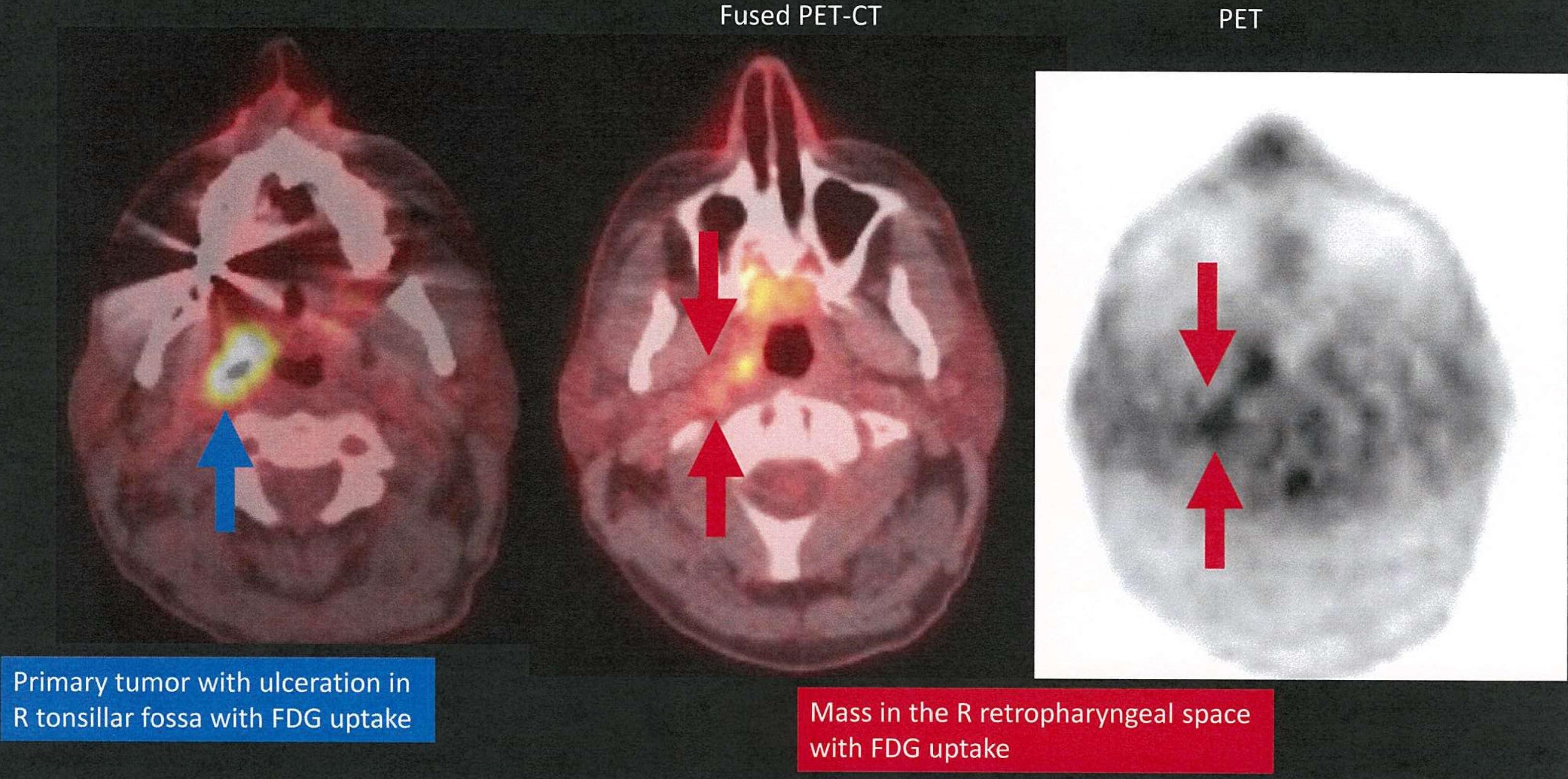
The following week the patient underwent a PET scan.
Join 6700+ physicians and attorneys on the email list.
The patient was referred to a head and neck surgical oncologist.
He underwent a right radical tonsillectomy and pharyngectomy.
During the surgery there were significant bleeding complications.
The tonsillar mass was removed, but the lymph node could not be addressed due to the proximity to the carotid artery. The surgery was aborted.
The patient was told that he would need a later operation to attempt removal of the lymph node.
This is where the critical error allegedly occurred. There was a failure of communication between the surgical oncologist, and the rest of the treatment team (local ENT, medical oncologist, and radiation oncologist).
From this point, the patient was treated as if the entire cancer had been surgically resected.
The patient was never brought back to the operating room to address the enlarged lymph node.
Pathology revealed HPV/p16-positive squamous cell cancer.
Operating under the assumption of complete surgical resection, the treatment recommendation was for radiation therapy but no chemotherapy.
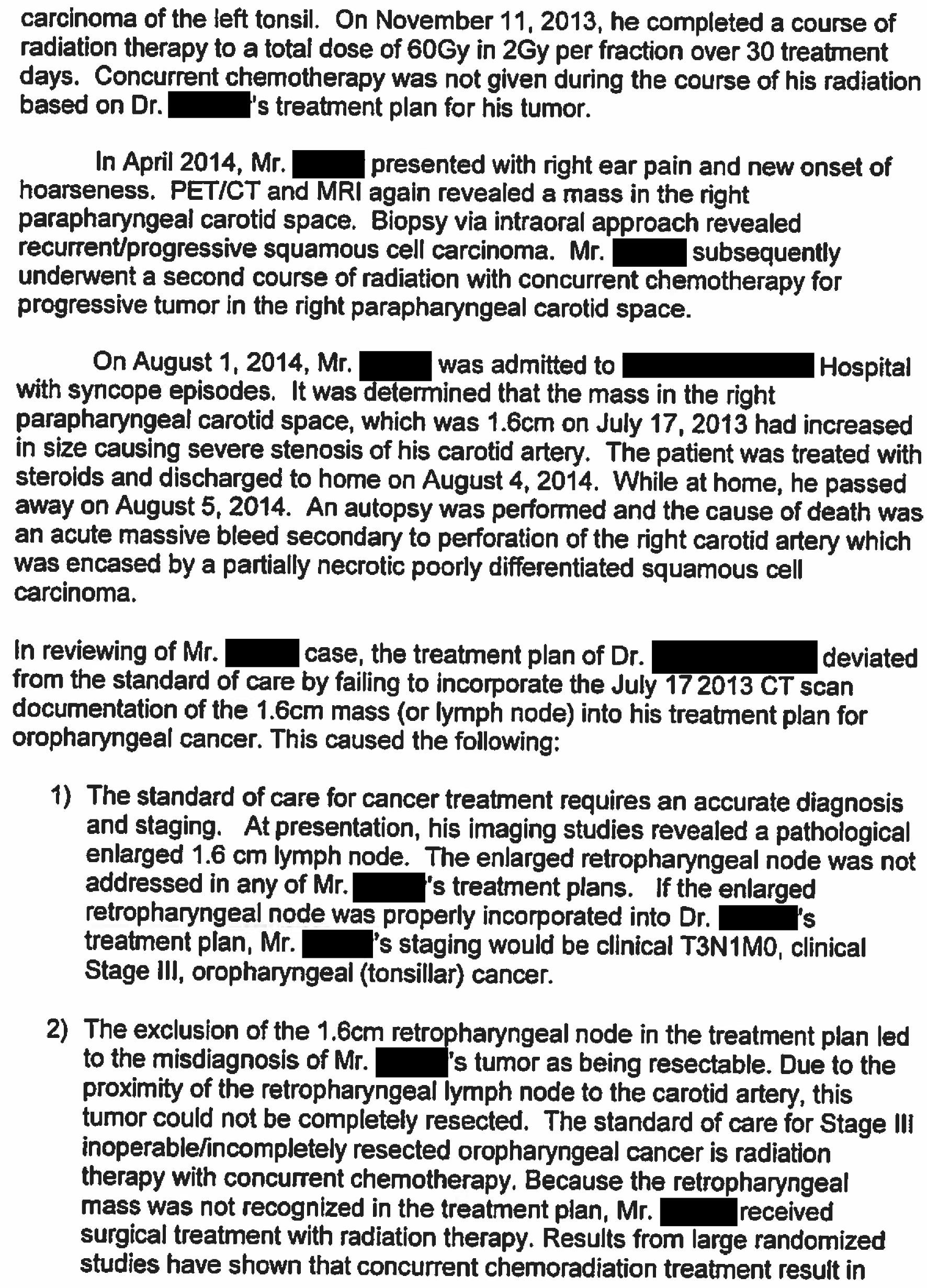
He underwent radiation therapy to a dose of 60Gy over 30 treatment days.
6 months later, the patient had worsening ear pain and difficulty speaking.
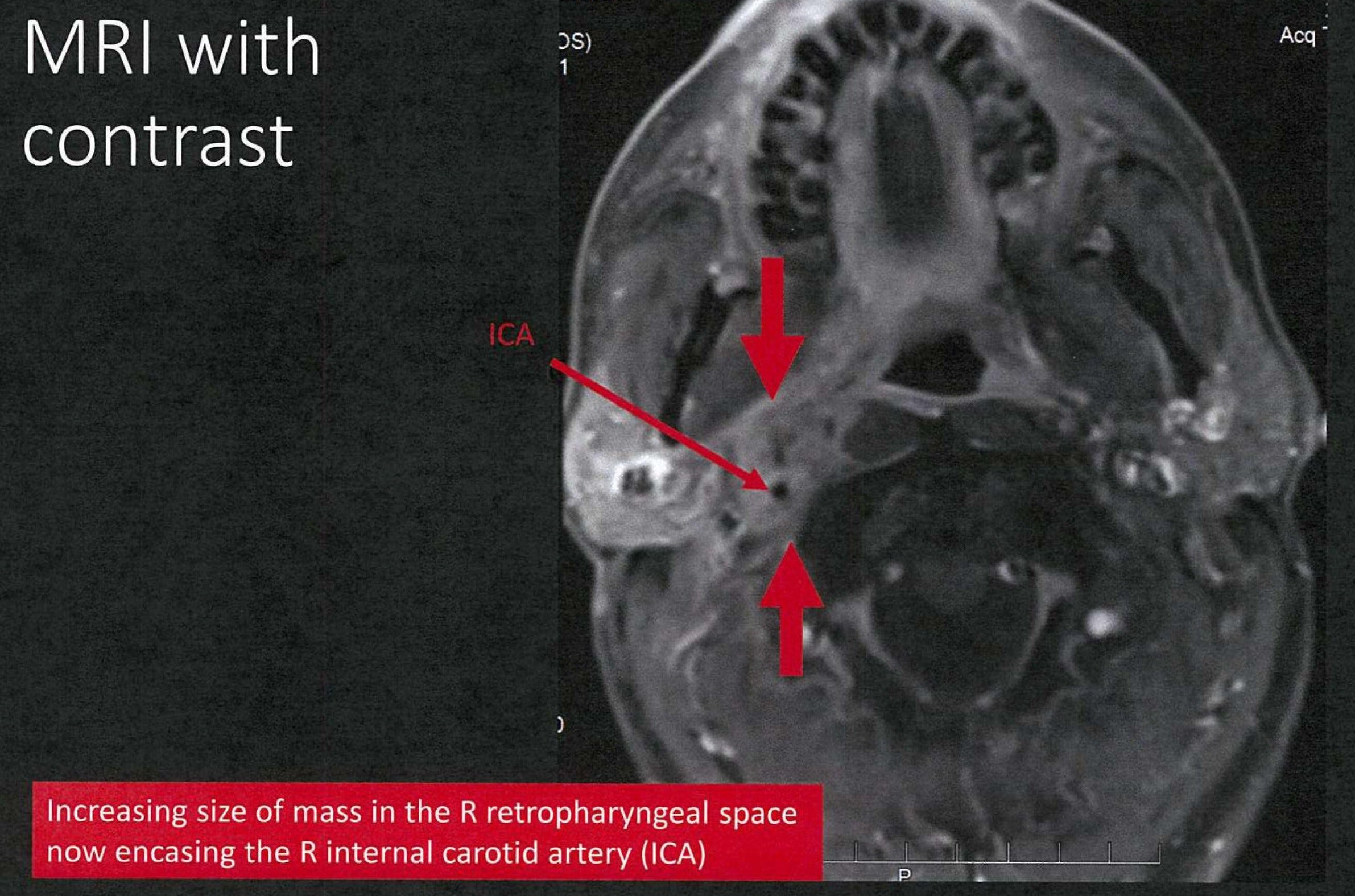
Repeat imaging showed recurrence of a mass in his right parapharyngeal carotid space.
Biopsy confirmed recurrent squamous cell carcinoma.
This time he underwent chemotherapy and radiation treatments.
4 months later, the patient presented to the ED with syncopal episodes.
Workup suggested that the lymph node had continued to progress, causing carotid stenosis.
The patient was hospitalized for 4 days and treated with steroids.
The day after he was discharged, he died at home.
The autopsy revealed he died of a massive bleed when the necrotic cancer in the lymph node eroded into his carotid artery.
This is also known as carotid blowout syndrome.
The patient’s family contacted an attorney, and numerous expert witnesses were hired to review his care.
The accusations against the doctors are described here:
Head and neck oncologist
Failed to communicate that the cancer was not completely resected
Failed to bring the patient back for a repeat operation
Radiation oncologist
Failed to realize that the tumor had not been completely resected
Gave radiation dose of 60Gy (only appropriate if completely resected)
Failed to give 70Gy (appropriate dose for remaining tumor)
Medical oncologist
Failed to give chemotherapy when indicated

The lawsuit was filed against the Ivy League hospital where the patient had his care.
The doctors were not named as defendants in the lawsuit.
The reason became apparent when the plaintiff filed their initial offer of compromise:

No physician has insurance coverage (nor personal assets) to cover this amount.
The reason they are requesting an astronomical amount became apparent in later court filings.
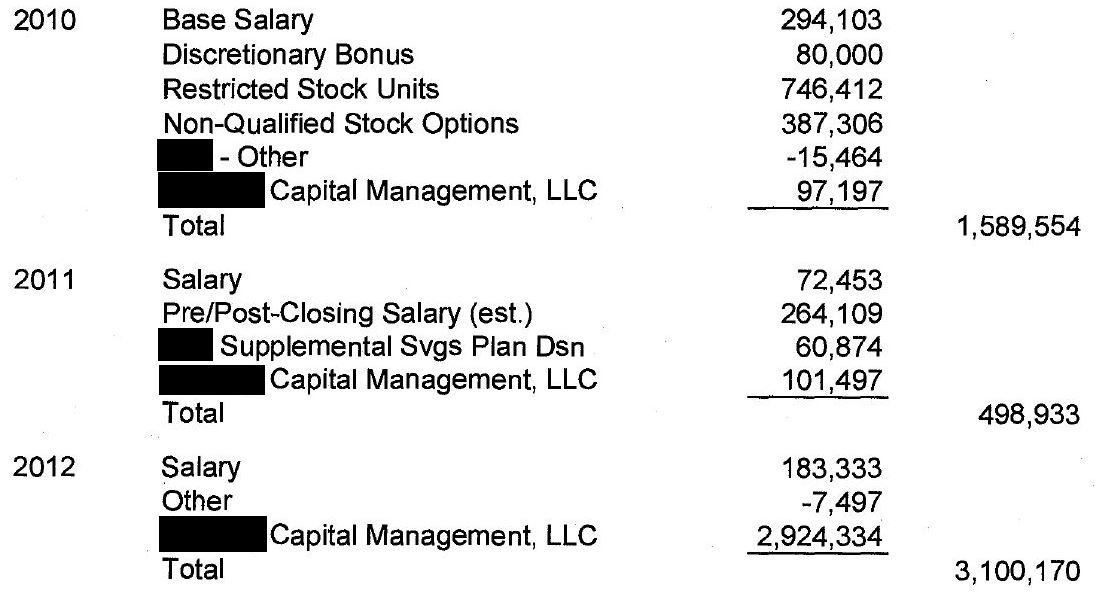
The patient was an extremely wealthy insurance executive and investor. His premature death meant the loss of a massive amount of earnings. As proof, the plaintiff filed records of his income.
The lawsuit reached an undisclosed settlement in early 2021. There was no trial.
Subscribe today for $180/year.
Readers will become medicolegal experts:
weekly review of new lawsuits
updates on active cases as they resolve
access to the entire archive.
MedMalReviewer Analysis:
This lawsuit is a good opportunity to review carotid blowout syndrome, a rare but feared complication of head/neck cancers. Here are two useful articles:
Prior to reviewing this case, I was not well-versed in the strong connection between HPV and squamous cell cancer of the head and neck. This is a key area in which vaccinations can reduce the incidence of cancers that have catastrophic outcomes.
The massive settlement offer will catch the attention of most readers. The plaintiff knows that the physicians will never be able to pay an 8-figure settlement, so instead they go after the hospital itself. The physicians simply becme pawns in a protracted legal game.