
Case #42

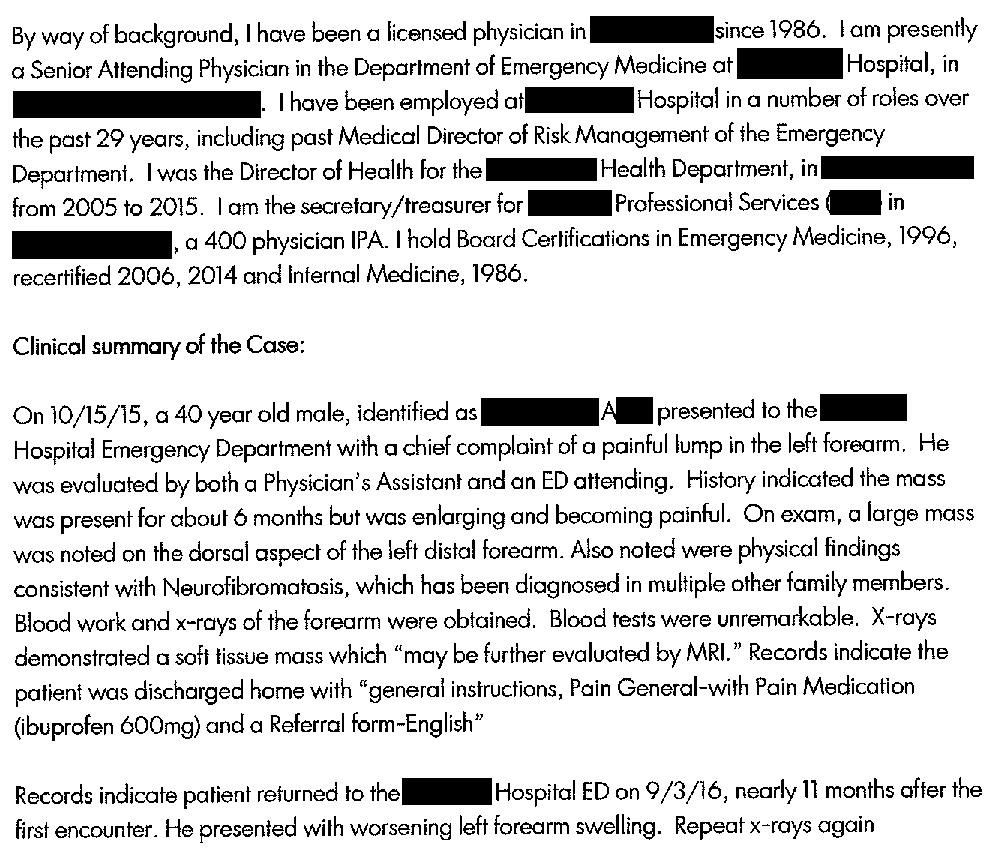
A 40-year-old man presented to the Emergency Department with a lump on his left forearm. He had first noticed it about 6 months ago and it had gotten progressively bigger.
Labs and an x-ray were ordered.
The x-ray showed a soft tissue mass and follow-up with an MRI was recommended.
He was told to follow-up with a PCP and discharged.
The patient did not follow-up.
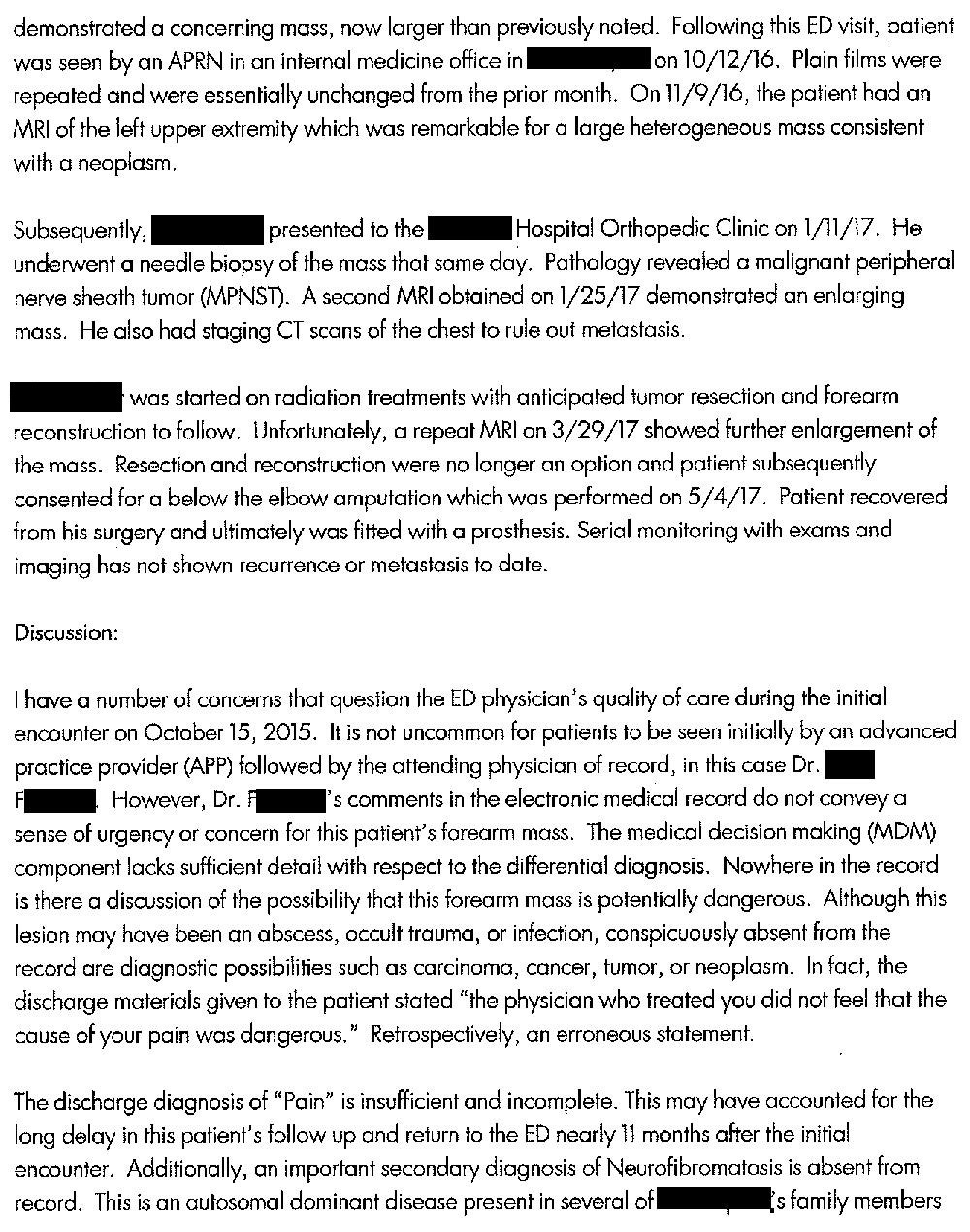
11 months later he went back to the ED, but this time was referred to an internal medicine clinic for follow-up.
An MRI was obtained showing a mass possible consistent with a neoplasm.
A biopsy was done, showing a nerve sheath tumor.
His left forearm was amputated.
Join thousands of subscribers.
Don’t miss out on learning pearls that will help you avoid malpractice lawsuits.
The patient hired a lawyer and a lawsuit was filed against the original ED physician, alleging inappropriate workup and follow-up.
An EM physician was hired to write an expert opinion.
Become a better doctor by reviewing medical malpractice cases.
Subscribe today to get a new case every week.
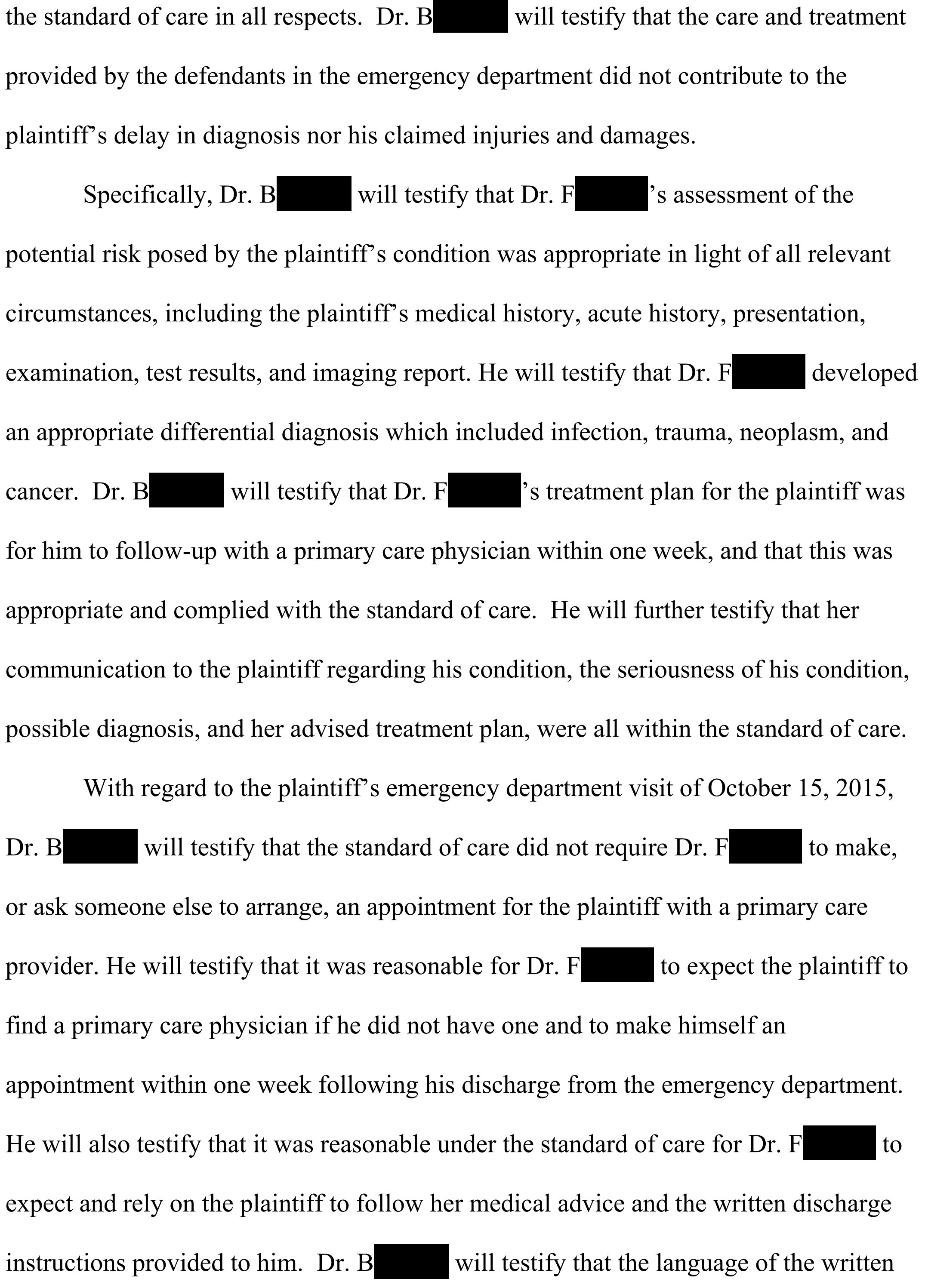
The defense hired an EM expert:

The defense also hired a neuropsychologist to point out that the patient had the mental capacity to contact a PCP and set up a follow-up appointment.

The plaintiff hired an orthopedic oncology expert (Dr. W) who charged $750/hr.
The defense hired an orthopedic oncology expert (Dr. T) who charged over $1,000/hr.
The plaintiff’s attorney wanted to depose Dr. T, but did not want to pay the higher fee.
They asked the judge to reduce Dr. T’s fees:

The judge rejected their motion, and allowed Dr. T to charge the higher amount.

Both sides reached a confidential settlement before trial.
MedMalReviewer Analysis:
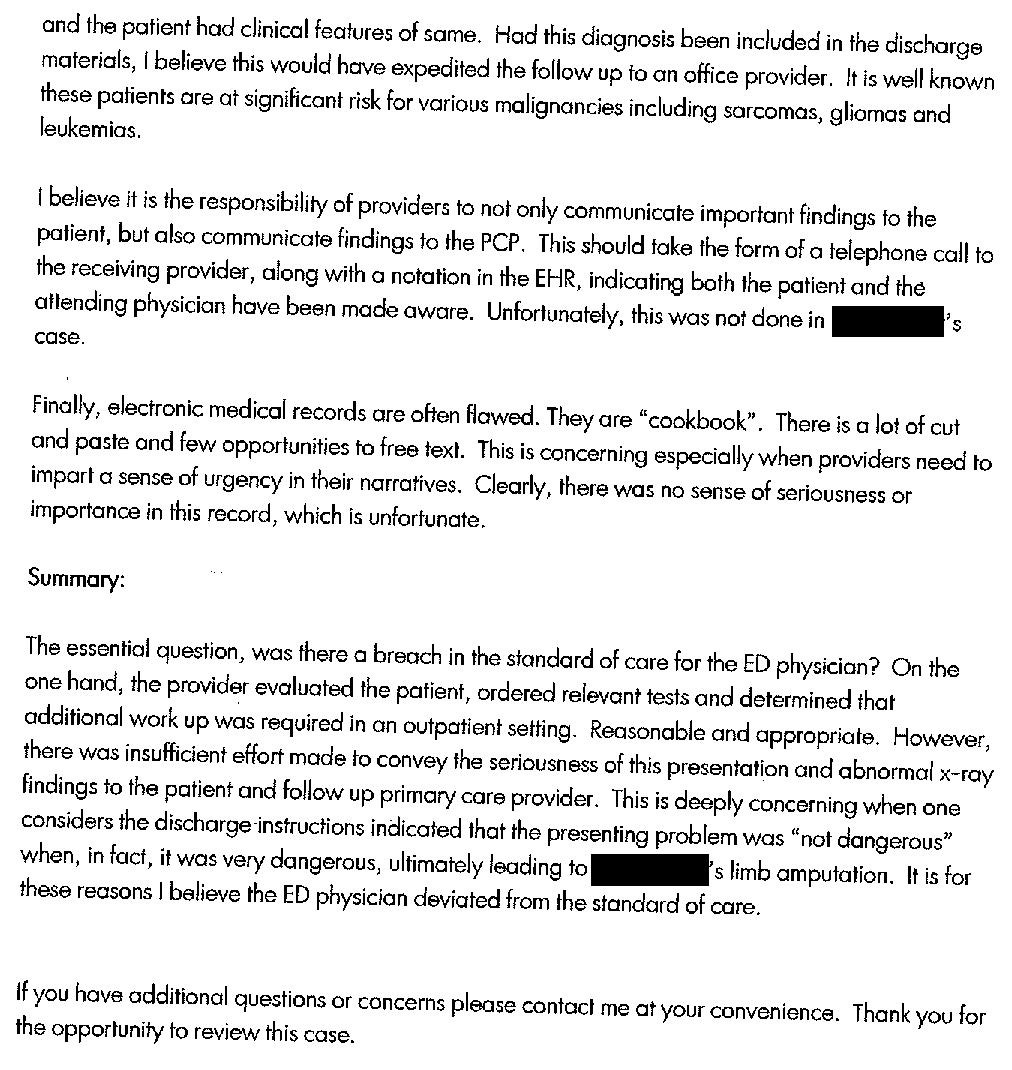
Lawsuits about incidental findings are common, but they mostly involve kidney or lung nodules. This case is unique because it involves a rare sarcoma on an extremity. The primary issue in many incidental finding lawsuits is a failure to tell the patient about the finding, but in this case the doctor got sued for not communicating the urgency of the follow-up.
The plaintiff has a valid point that saying this problem was “not dangerous” was wrong, but nonetheless he still should have followed-up with a PCP. Providing a patient a phone number to call for follow-up meets the standard of care in my assessment. However, I will note that patients often think that a “referral” means that they will get a phone call to schedule an appointment. I’m in the habit of telling most patients that they must call themselves to set up an appointment.
This expert opinion is actually written by a physician. Many opinions are written by a lawyer and rubber-stamped by the doctor. The language in this piece makes it obvious that it was written by a medical professional.
Communication is critical in incidental findings. Not only do you need to explicitly warn the patient about the finding, you need to thoroughly document that you had a discussion including the serious adverse effects if it is ignored. Making a phone call to the patient’s PCP is wise, but it goes above the typical expectations in the ED.
Case #39: Missed tongue cancer [Subscribe to Read]
Specialty: ENT
Synopsis: Man with chronic sore throat and ear pain has mass on posterior tongue on CT scan. ENT does nasal endoscopy but sees nothing suspicious.
Case #40: Operation on wrong side of head
Specialty: Neurosurgery
Synopsis: 53-year-old man has a large MCA stroke. Taken to OR for decompressive hemicraniectomy, but they accidentally operate on the wrong side.
Case #41: Iatrogenic Overdose [Subscribe to Read]
Specialty: General surgery
Synopsis: A man in his 60s develops diverticulitis with abscess. He is given multiple escalating doses of Dilaudid, and eventually found apneic with severe anoxic brain injury in his hospital bed.
ED doc here. I disagree with the expert witness reviewer. The ED provider may have been wrong to indicate the finding was not dangerous, but the ED provider made the appropriate recommendation to follow up with the PCP. In effect, the ED provider discharged the responsibilities of followup to the patient. If something catastrophic had happened within 2-4 weeks of the ED discharge, it would be reasonable to lay some blame on the ED provider. 11 months? That is well beyond the responsibility of the ED which, lets not forget, exists for immediate care of imminently life or limb-threatening disease.
This disease was ultimately serious. This disease was not serious when the patient first presented to the ED. The patient was given adequate instruction to go to an appropriate followup. The patient didn't do it. No fault rests with the ED provider here.
This is insane. 11 months later and they try to hold the ED doc responsible for the patient not following directions to follow up with their pcp?
In my discharge summary and MDM I'll often use the phrase, "fortunately no dangerous emergency condition was identified today but it is still important that you are closely followed by your pcp (or other relevant followup)" and then I'll actually order a follow-up for 3-7 days through our referral system. We are fortunate to have this in 2023. Maybe what I should use for phraseology instead is, " fortunately no imminently life threatening condition was identified today but... "?
What an absurd profession we have where lay people who have no clue (including their lawyers) invent asinine standards of care that are completely impractical in our deteriorating practice environment.
Is the insinuation that on night shift in completely overburdened hospitals boarding 30 to 130 patients in the ED, that I should admit this patient overnight for urgent morning MRI?!