


Central Pontine Myelinolysis
Case #211
A 64-year-old woman with a history of SIADH was scheduled to see her endocrinologist (Dr. B).
Labs were drawn, and her sodium level was 118 mmol/L.
She was noted to have altered mental status, dizziness, and balance issues.
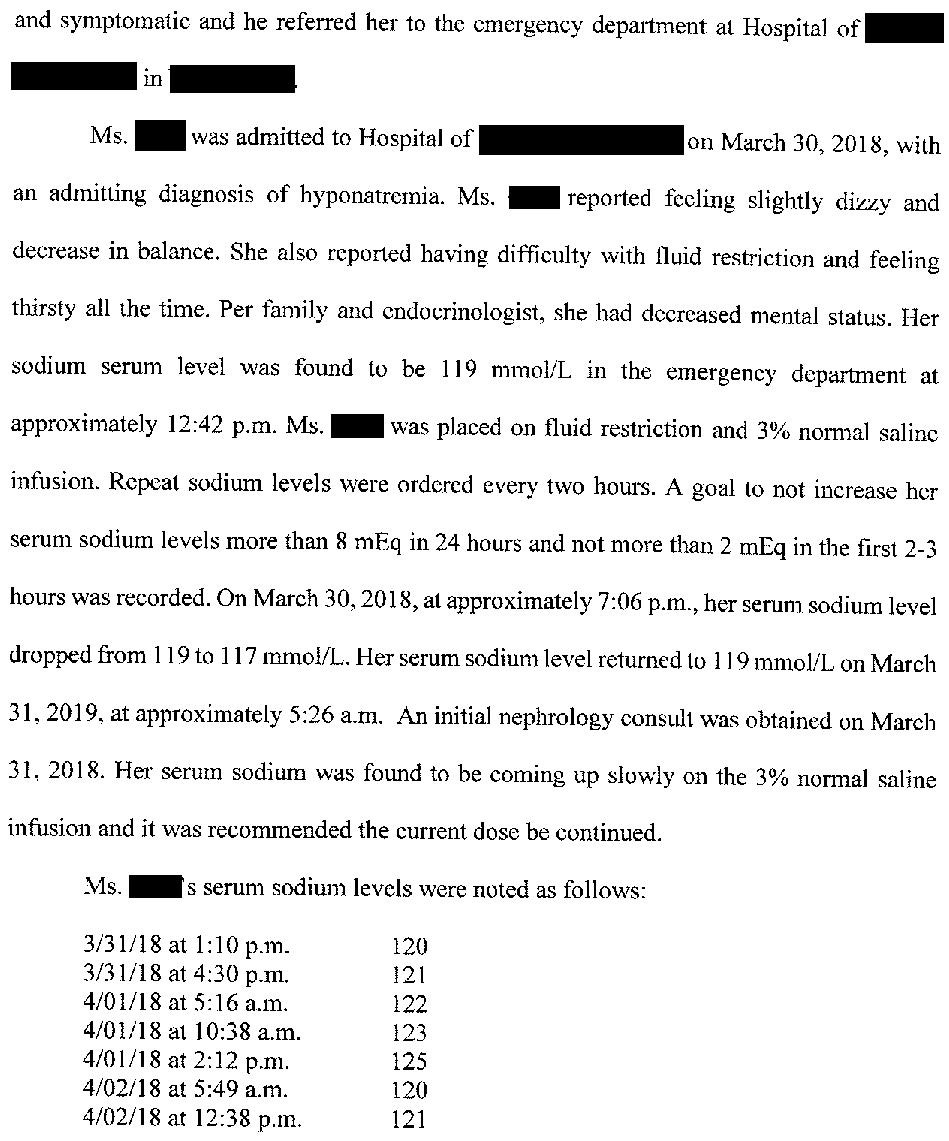
After the appointment, she was directed to the ED and admitted.
The hospitalist (Dr. S) consulted nephrology (Dr. F) and started 3% normal saline at 30mL/hr.
Over the next few days, her sodium hovered in the 120-125 mmol/L range.
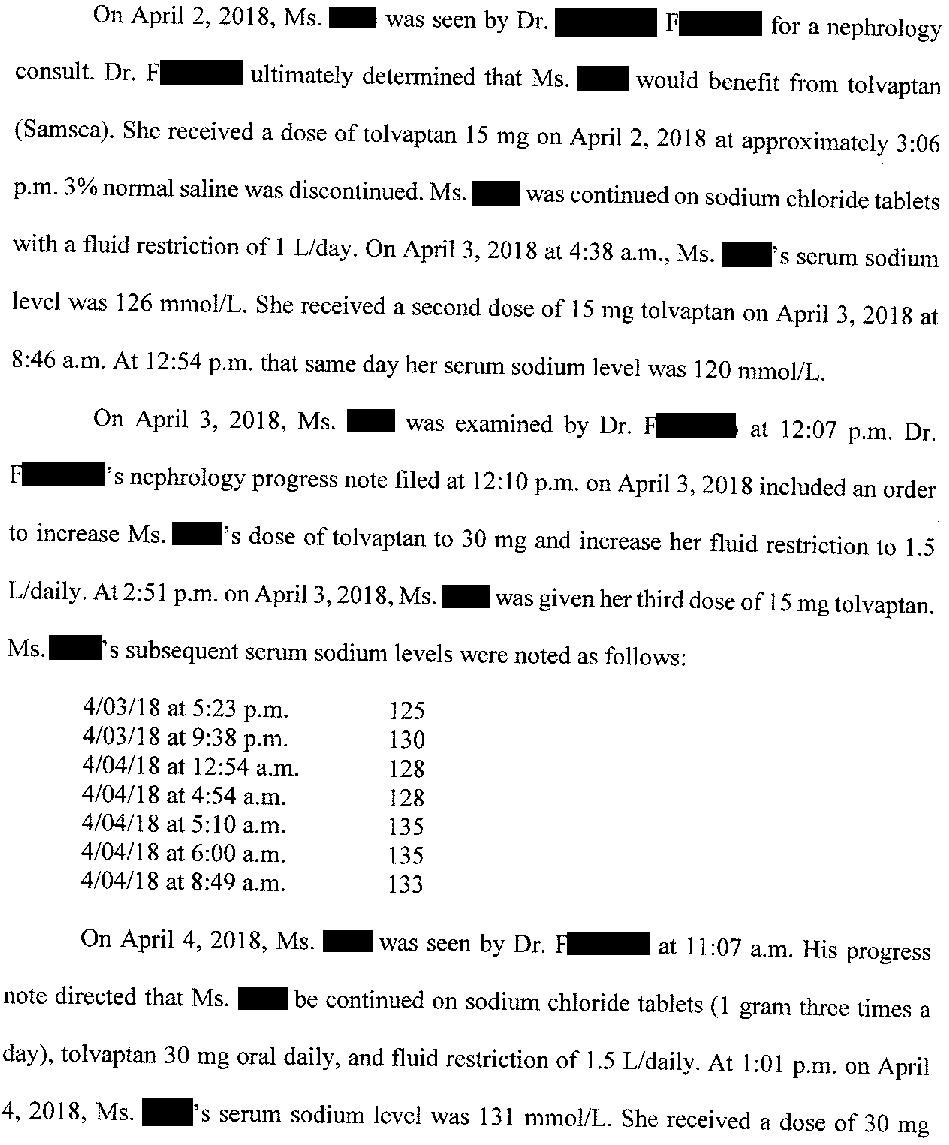
On day 4 of hospitalization, the nephrologist recommended stopping 3% normal saline, starting 1g NaCl tablets TID, starting tolvaptan 15mg qday, and continuing a 1.5L fluid restriction.
Don’t miss the Anniversary Sale!
New annual subscriptions are 20% off.
The following day, her sodium had increased to 126 mmol/L.
Dr. F recommended increasing tolvaptan to 30mg qday.
The next morning, her sodium was 133 mmol/L.
The patient was discharged home.
After being home for one day, the patient’s husband note she was confused and acting abnormally.
He called the endocrinologist (Dr. B), who ordered outpatient labs be done the same day.
The sodium level came back at 152 mmol/L.
Dr. B saw the results the next morning, and told the patient’s husband to take her to the ED.
The sodium was 170 mmol/L.
She had altered mental status and balance issues.
Her symptoms persisted despite normalization of her sodium.
3 weeks later, an MRI scan showed signal abnormalities in the pons.
She was diagnosed with central pontine myelinolysis.
The patient’s family contacted a law firm and filed a lawsuit.
The hospitalist, nephrologist, and endocrinologist were sued.
The plaintiff’s nephrology expert wrote the following opinion:
The plaintiff also hired an endocrinologist expert witness (both the expert and the defendant are named Dr. B).
Improve your practice and become a medicolegal expert.
An annual subscription will never be cheaper, subscribe today to save.
The defense responded with their own nephrologist:
The plaintiffs offered to settle with the endocrinologist for $1,000,000.
They offered to settle with the nephrologist for $2,500,000.
No offer was made to the hospitalist, and she was removed from the lawsuit within several months of the initial filing.
After 4 years a confidential settlement was reached with the endocrinologist and nephrologist, and the lawsuit was withdrawn.
MedMalReviewer Analysis:
The allegations against the endocrinologist seem particularly unfair. He was not involved in the medication decisions that resulted in her rapid sodium changes. All he did was agree to see the patient in follow-up a week after discharge. He was criticized for failure “to educate himself prior to assuming responsibility for following the patient while on tolvaptan” when he was simply trying to help monitor the patient and continue her new prescription. In fact, he seemed very attentive when her husband called. He ordered outpatient labs, reviewed the results, and appropriately referred her to the ED all within <24 hours. His actions indicate that he is a thoughtful, responsible, caring doctor. The expert witness who criticized him is unprofessional and incompetent.
Before reading this case, I had only considered central pontine myelinolysis as a possibility in the context of rapid elevation of hyponatremia back to a normal sodium level. However, it seems to have happened with a rapid escalation from a normal sodium level to hypernatremia. This case has helped me expand my mental model of this disease process.