


Chronic neck pain leads to parapegia [EM, Neurosurgery]
Case #54

A woman in her 50s presented to the ED on February 19 with neck pain for 2 days.
She had a history of anterior cervical discectomy and fusion done several years earlier by Neurosurgeon #1.
A cervical neck x-ray revealed no acute abnormalities, she was given trigger point injections, and discharged.
She presented back to the same ED the following day, no imaging was obtained, and she was again discharged.
She then followed up with her PCP, who ordered an outpatient non-contrast cervical spine MRI. It was completed on February 23, and showed abnormal soft tissue at C7-T1, “most likely representing an extruded and migrated disc fragment”. The radiologist recommended repeat scan with contrast.
The contrast scan was completed 3 days later on February 26. The radiologist’s report noted:
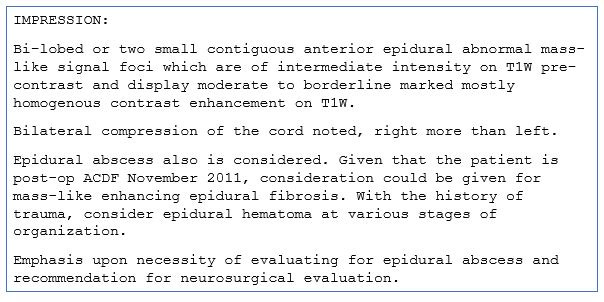
The radiologist called the PCP, who was able to contact both a neurosurgeon and the patient to arrange rapid referral.
The patient saw the neurosurgeon (Neurosurgeon #2) the next day, February 27. He reviewed the MRI results, but felt that her symptoms were primarily due to cervical radiculopathy and did not recommend any intervention or treatment.
About 2 weeks later the patient went back to the ED with shoulder pain. Chronic neck pain was also noted.
She was seen by a PA, supervised directly by a physician.
No imaging of the neck was obtained.
The PA copy/pasted the prior MRI impression into the note, except for the part mentioning possible epidural abscess.
The patient mentioned she had a second opinion with another neurosurgeon the next day.
She was discharged from the ED.
The patient saw the next neurosurgeon (Neurosurgeon #3) on March 18.
He noted the epidural finding on the MRI, but with no neurologic deficits, did not think it was infectious.
He suspected a residual hematoma from her previous surgery.
She was told to follow-up with the original neurosurgeon, Neurosurgeon #1, who did her ACDF.
On April 14, the patient awoke with loss of bladder control and weakness in her legs.
She was taken back to the ED, and a repeat MRI revealed a definitive epidural abscess at C7-T2.
Neurosurgeon #2 was on call that day, and performed a decompression.
Her hospital course was complicated by sepsis, respiratory failure, renal failure, pulmonary emboli, tracheostomy, decubitus ulcers.
She was left with hand weakness, no sensation below T1 dermatome, and complete paralysis of lower extremities.
Join 6100+ doctors and lawyers.
Subscribe today.
The plaintiff filed a lawsuit against the hospital, both neurosurgeons, and their employers.
Of note, none of the ED clinicians were specifically named as defendants. The last ER doctor to see the patient, as well as 2 PAs working in the ER were listed in the lawsuit as agents of the hospital.
The plaintiff hired EM and neurosurgeon expert witnesses.
The EM expert wrote the following opinion:
A neurosurgeon also wrote an opinion:






The lawsuit was filed in February 2015.
After extensive legal maneuvering, the case finally resolved 4.5 years later.
It was settled for a confidential amount.
MedMalReviewer Opinion:
I strongly disagree with the EM expert’s criticisms of the ED physician and mid-levels. The care they provided was appropriate. The patient had already seen a neurosurgeon for the MRI findings and had a second opinion set up for the following day. There was no indication to obtain another MRI or admit her to the hospital, given she had no signs of acute spinal cord compression. She simply had chronic neck and shoulder pain.
The EM expert’s suggestion that the neurosurgeon should be consulted for chronic pain (absent any new neurologic changes) is inaccurate. This would lead to a truly astonishing number of consults without any benefits.Copy and pasting radiology results into the medical record is unnecessary. These results are already included in the medical record elsewhere, duplicating them in your note offers no medicolegal protection. Simply describe a summary of the findings and how they influence your decision-making.
However, if you insist on copy/pasting, include the entire impression. Removing various parts only makes your case harder to defend when you miss something important.The fact that 2 separate neurosurgeons gave similar opinions is beneficial to the defense. It suggests that they both were operating within the standard of care. Nonetheless, patients with catastrophic injuries are risky to take in front of a jury, so these cases usually settle prior to trial.
Steven Shroyer, M.D., November 21.
There are, and i expect there will be some more cocky responses to this presentation, stating malpractice was committed. The fact is, missing the dx of pyogenic spinal infection on a patient’s first visit to the ED has been the standard of care for the past 25 years (75% miss rate, Davis et al, JEM 2004, 66% miss rate, Shroyer, et al WJEM 2021). Anyone stating they’d would have diagnosed it when 75% of physicians do not, is quite frankly arrogant. Until there is a high quality risk prediction tool that is sensitive yet avoids over imaging patients—which risks exposure to radiation, over boarding in the ED, and gadolinium contrast—physicians in all specialties will continue to miss this diagnosis. Evidence is limited but screening patients with back or neck pain for the 10 Davis risk factors and then using a CRP level to decide on imaging is the most accurate approach in evaluating patients with neck or back pain who are being considered for the diagnosis of pyogenic spinal infection (Davis WT, et al. CJEM, 2020). Anyone evaluating patients with back or neck pain, including PAs, nurse practitioners, emergency physicians, hospitalists, and neurosurgeons should inform themselves of this. The only physicians I’ve seen routinely not miss this diagnosis are infectious disease specialist. This is because patient selection before they are consulted allows them to see more cases than any other specialty. In my career, I have evaluated more than 90 PSIs and missed more than five, four which either died or suffered devastating neurologic consequences. It is a very humbling diagnosis. Thankfully it’s low incidence of one per thousand back pains limits even more devastating misses and medical legal catastrophes.
Red flags all over the place. Ignoring the MRI report was a real problem but this case also reveals the issue of consultants not willing to come to the ED when consulted. I’m amazed how often this happens and they get away with it most of the time but it bit them in the butt this time. I once had a surgeon refuse to see a sick patient with free air in the abdomen on CT. I didn’t accept that and with much pushing got the guy to come in and take the patient to the OR for his perforated ulcer.