


Hand Compartment Syndrome [IV infiltration]
Case #49

A middle-aged man was scheduled for a colonoscopy.
In the pre-op area, an IV was started in his right hand. It was not working properly, so an IV was started in his right antecubital fossa.
The nurses started fluids through the IV, and the patient continued to have pain.
Nurses reassured him that the IV was working well.
In the colonoscopy suite, the anesthesiologist pushed a bolus of propofol.
He returned several minutes later and the patient still had a normal level of consciousness.
The anesthesiologist determined the IV was not working, and he started a line on the patient’s left hand.
The new IV worked well, and the colonoscopy was completed without issue.
After he woke up, the patient still had severe right hand and arm pain.
The patient and his fiancé requested a physician evaluate the pain.
The GI physician came to the bedside and reassured him that it would improve
The patient was discharged home.
The following day the patient still had severe right arm pain.
He went to the ED, was diagnosed with compartment syndrome, and taken to the OR for fasciotomies.
The patient developed complex regional pain syndrome (CPRS) and has permanent dysfunction of his right arm.
The patient contacted a lawyer and a malpractice lawsuit was filed against the anesthesiologist, the GI doctor, and the hospital.
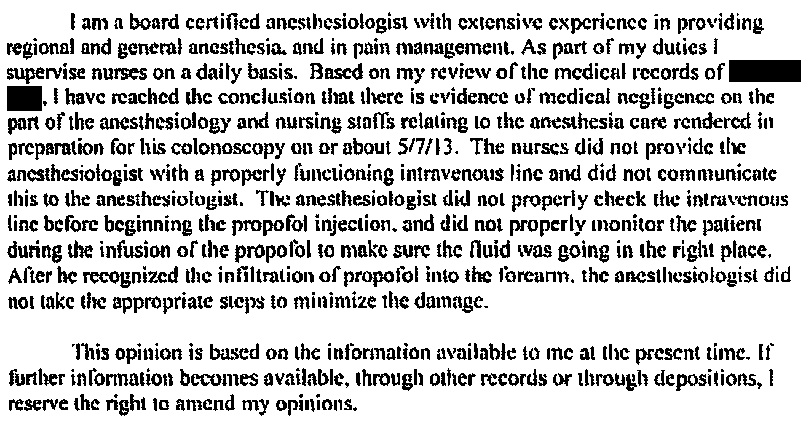
The plaintiff’s anesthesiologist expert wrote the following opinion:
The anesthesiologist felt strongly that he had not breached the standard of care. A defense expert was hired to counter the plaintiff’s claims.

The plaintiffs also hired a GI expert witness:


The defense countered with their own GI expert:

The plaintiff offered to settle the case for $3.95 million.

The lawsuit was withdrawn after a confidential settlement was reached.
It took 3.5 years from filing to settlement.
MedMalReviewer Opinion
This case involves both plaintiff and defense experts from 2 different specialties. Its rare to find defense expert opinions, and I’ve been saving this case for paying subscribers only. Seeing both sides of the lawsuit gives a better perspective.
Disabling injuries that are not fatal lead to the highest settlements, often even higher than fatal mistakes. Compartment syndrome of a hand is a good example. Other common examples include birth injuries and spinal epidural abscesses.
Severe pain should always raise a red flag for compartment syndrome, which necessitates emergency evaluation. I’ve seen several similar cases from IV infiltration in various settings, including by EMS.