


Intubation Fiasco [Bowel Obstruction]
Case #60

A 75-year-old woman presented to the hospital ED on New Year’s Eve, 2013.
She reported abdominal pain and distension, nausea, and lack of appetite.
A CT scan was obtained showing a small bowel obstruction.
An NG tube was placed and surgery was consulted.
The following morning she was feeling slightly better.
The NG tube was removed.
On January 2nd, she had increasing pain and nausea.
The surgeon charted that the patient “failed conservative management”, ordered that the NG tube be replaced, and took her to the operating room.
The patient’s intubation did not go well.
Both an anesthesiologist and a CRNA were present.
The NG tube had not been replaced prior to the intubation attempt.
A massive wave of vomit flooded her airway.
The airway was secured but not before she aspirated a large amount of fluid into her lungs.
The surgery was completed but over the next 10 days she slowly declined.
She eventually developed multi-system organ failure and tragically passed away.
The patient’s family contacted a law firm and filed a lawsuit against the hospital, the surgeon, the anesthesiologist and the CRNA.
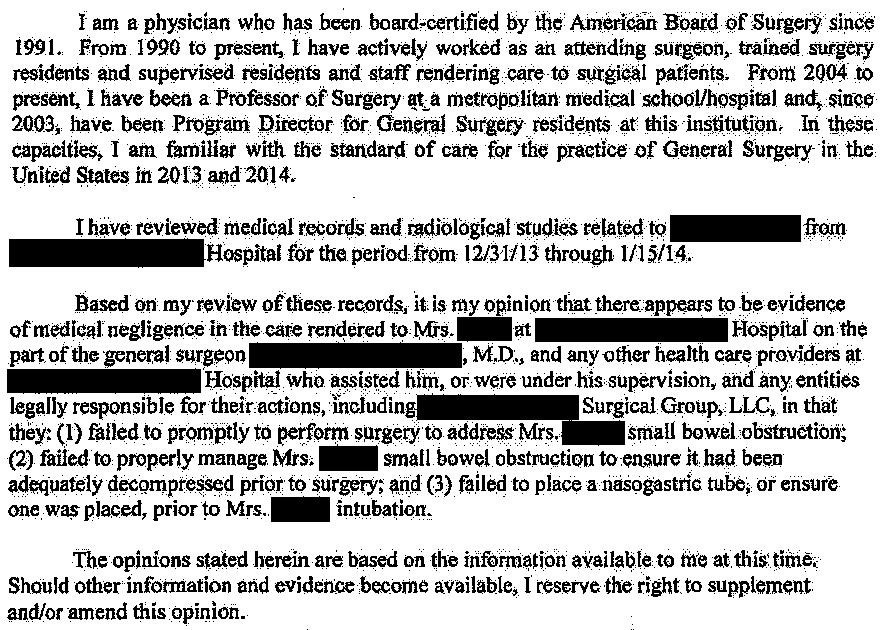
An anesthesiologist was hired to write an expert opinion:

Join 6300+ doctors and lawyers.
A general surgeon was hired as an expert witness:
Subscriber Benefits:
A new medical malpractice case each week.
Access to the complete archive of 60+ cases.
Updates as ongoing lawsuits progress.
Insights from cases involving nearly every specialty to build a broad base of medicolegal expertise.
The plaintiffs offered to settle the case for the following amounts:
Surgeon: $6,000,000
Anesthesiologist and CRNA together: $6,000,000
There was no documented offer of compromise to the hospital.
The case reached a confidential settlement from all parties.
MedMalReviewer Analysis
Both the anesthesiologist and the CRNA were named as defendants. Simply having a supervising physician present does not necessarily result in liability protection for non-physician practitioners.
The plaintiffs know that a hospital has deeper pockets than an individual physician, and therefore have strong incentive to name the hospital as a defendant. In this case, the hospital is being sued due to the alleged negligence of it’s agent (the nurse) in not placing the NG tube. However, no nurses were specifically named as defendants.
When a plaintiff offers to settle a case, their initial offer is usually quite high. The offers for compromise in this case go far above any reasonable level. The patient’s remaining life expectancy was short, which likely resulted in a settlement that was a tiny fraction of the $12,000,000 total requested.
Question
Say that you were asked to make a ruling on who was responsible for this bad outcome. What percentage of the liability would you assign to each of the following parties?
the nurses
the surgeon
the anesthesiologist
Check out these recent cases:
Brain Abscess [Subscribers Only]
Specialty: Neurosurgery
Synopsis: ED misses brain abscess, admits patient with unclear diagnosis. Neurologist orders MRI revealing brain abscess with midline shift, neurosurgeon delays operation.
Specialty: Orthopedics
Synopsis: Patient undergoes left reverse total shoulder arthroplasty, axillary artery is injured, poor outcome despite emergency vascular repair.
Specialty: Psychiatry
Synopsis: Patient admitted for suicidal thoughts and substance abuse. Discharged after improvement, but commits suicide 10 days later. Family alleges that patient should have been sent directly to substance abuse treatment.
No reason the nurse should be liable
The CRNA and anesthesiologist should have recognized that the stomach needed to be decompressed before intubation.
I'm surprised most commenters seem to fault the anesthesiologist/CRNA for not placing an NGT
(insert blame anesthesia joke here). In my experience this is the responsibility of the primary surgical team. That being said if a patient came to me who I thought needed an NGT prior to induction, I would absolutely not proceed until the surgical team had done so. I have yet to encounter a situation where the surgeons were not amenable to this after discussion.