


Paralyzed Patient [Missed Thoracic Stenosis]
Case #117

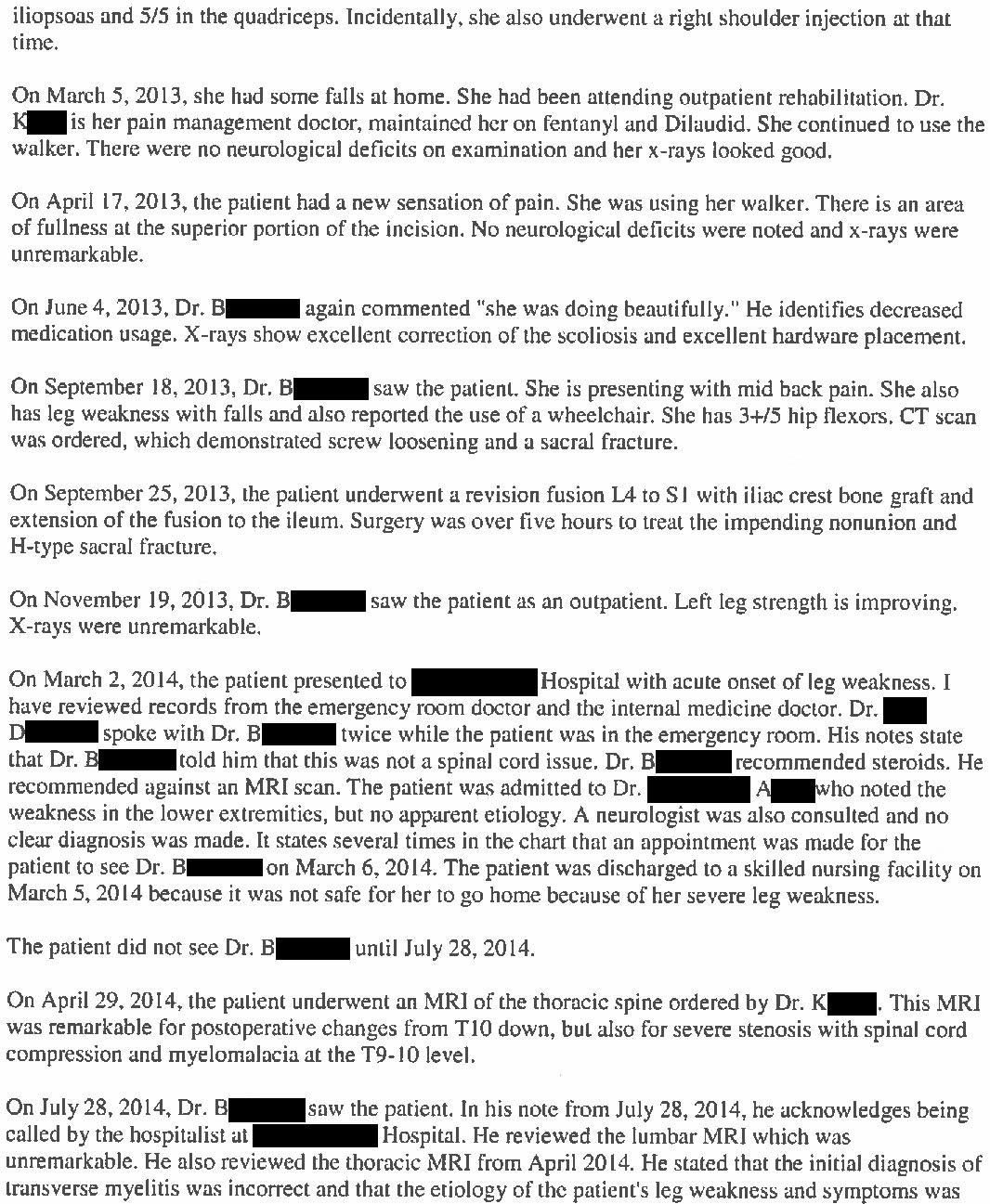
A 65-year-old woman presented to the ED on March 2, 2014 with acute bilateral leg weakness.
She had a history of degenerative scoliosis and lumbar stenosis.
Her past surgical history included 2 prior spine surgeries:
lumbar fusion in November 2012
revision fusion in September 2013 due to screw loosening and a sacral fracture
Both surgeries were done by the same ortho spine surgeon (Dr. B).
The ED physician (Dr. D) saw her and consulted her spine surgeon.
The spine surgeon recommended steroids and outpatient follow-up.
The ED physician specifically asked to get an MRI, but the spine surgeon did not feel it would be helpful due to the hardware in her lumbar spine.
The patient was unable to walk, therefore the ED physician admitted her to the hospitalist (Dr. A).
In the hospital, a neurologist was consulted (Dr. P).
The neurologist ordered an MRI of the lumbar spine.
It did not show any explanation for her weakness.
The neurologist felt she was improving with steroids but could not identify an exact explanation for her symptoms.
The differential included transverse myelitis and conversion disorder.
The patient was in the hospital for 3 days, then discharged to rehab.
A follow-up appointment was scheduled with her spine surgeon the day after discharge.
She did not make it to that appointment, presumably due to the logistical difficulties surrounding the discharge from the hospital to rehab.
Her care at the rehab facility was managed by Dr. K, an internal medicine physician.
He requested another neurology consult, and she was seen by Dr Y after being at the rehab center for about 6 weeks.
Dr. Y ordered an EMG, which was normal.
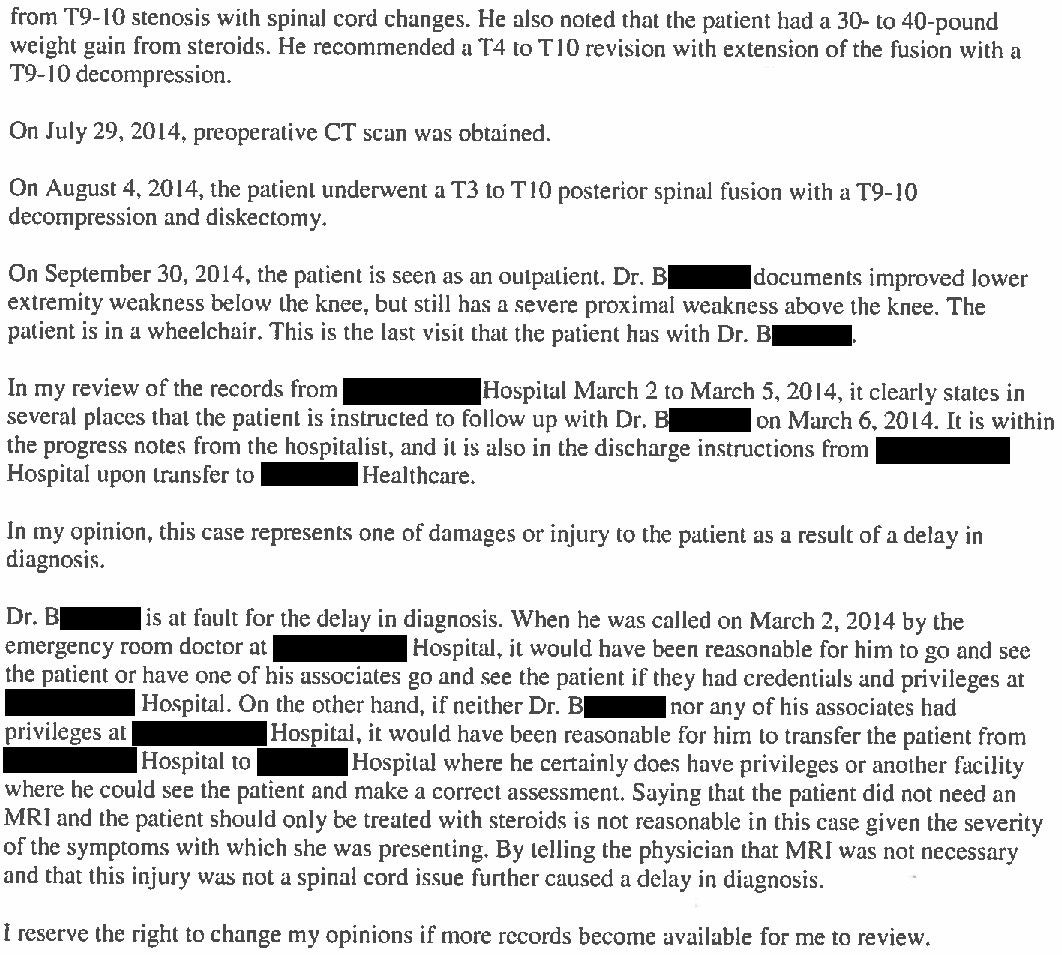
Dr. Y ordered an MRI thoracic spine, which was completed 5 days later.
The MRI results are shown here:
“T9-T10 bilateral paracentral disc protrusion superimposed on a circumferential disc bulge, significant mass effect on the thoracic spinal cord. This is considered a moderate to severe stenosis. Questionable faintly increased signal in the substance of the spinal cord, possibility of edema.”
The radiologist did not attempt to contact the ordering physician or flag it as a critical finding.
Unfortunately, Dr. K (rehab IM doctor) did not understand the significance of this finding and documented that it was a “normal” MRI.
Dr. Y (neurologist who requested the thoracic MRI) apparently never saw the patient again nor followed-up on the MRI result.
The patient was discharged from rehab after 90 days, in June 2014.
She was moved to an assisted living facility.
She still could not walk.
She followed up with her PCP about one month later.
The PCP reviewed the thoracic MRI and realized that she had been suffering from spinal cord compression this entire time.
He immediately called her spine surgeon (Dr. B) to notify him.
Dr. B saw her 2 weeks later and recommended a thoracic decompression.
A week later she finally underwent thoracic decompression at T9-T10 and T3-T10 fusion.
The patient ultimately regained some strength distal to her knees, but still has severe proximal weakness.
She permanently uses a wheelchair.
My research shows she now lives in an assisted living center.
She serves as the president of the resident’s council at the facility and is very active in the community.
Join 7500+ doctors and lawyers on the email list.
I dig through thousands of med mal cases to bring you insider information, real-life expert witness opinions, and learning pearls that you’ll actually remember.
The patient was understandably upset about this series of events.
She filed a lawsuit against all of the physicians except the ED physician and her PCP.
The radiologist who read the thoracic MRI was also named as a defendant.
An IM expert witness was hired to criticize the rehab doctor (Dr. K) for not acting on the thoracic MRI report:
A ortho spine surgeon was also hired as an expert witness:
The defense discussed the case with several experts, but did not disclose these opinions.
They realized this would be a very challenging case to defend.
It was settled on behalf of all defendants.
The amount is confidential.
MedMalReviewer Analysis:
In my opinion, the number one learning point from this case is to remember to check the thoracic spine if the lumbar spine is negative. I’ve seen this mistake made numerous times by EM, neurology, hospitalists, PCPs, and spine surgeons. A common mental error is to fixate on the previous operative interventions in the lumbar spine and fail to consider a new lesion.
The ED doctor consulted the spine surgeon and followed his advice, to the patient’s detriment. Specialists offer expertise that is critical for providing good care, but we also have to be cognizant of the fact that they can be wrong. Consulting a specialist is not a license to stop thinking.
If your hospital requires board-certified EM physicians to get permission for spine MRIs on patients who have objective red flags for spinal cord compromise, it operates below the standard of care. In fact, this hospital was sued for not having appropriate procedures in place:

The appropriate workflow for these orders should involve simply placing the order in the EMR. Additional phone calls or consults are unacceptable barriers. If your hospital does not have acceptable protocols for ED spine MRIs, its simply a matter of time until patients are paralyzed, the hospital will be sued, and the hospital will lose a large sum of money. These outcomes are rare enough that most administrators are unaware of the risk, but common enough that many hospitals every year lose millions of dollars and garner negative publicity. Be warned.
It’s reasonable to start with a lumbar MRI. Its often where the problem lies. However, you need to have a quick reflex to add on the thoracic MRI if the lumbar is negative. You should tell the MRI techs this before they start the scan. Alternatively, simply order both the thoracic and lumbar at the same time. While I’ve never seen a lawsuit from a missed cervical lesion, there is a reasonable argument to scan the entire spine. Epidural abscess frequently present with skip lesions and the neurologic exam may not be as reliable to localize as we were taught in medical school.
Another issue highlighted by the defense is the radiologist’s failure to contact the ordering doctor about the new thoracic lesion. It sounds like the images looked concerning but were not clearly emergent. The rehab doctor clearly failed to understand the significance of the MRI results. Direct conversation between the two could have been helpful. Furthermore, the neurologist who recommended the MR didn’t follow up on it.
Spinal stenosis from a bulging disc is actually somewhat of a difficult concept to grasp for people who aren’t spine specialists. Often we’re looking for the big, acute, dramatic finding… an epidural abscess, spine hematoma, giant metastatic lesion, etc… But these spinal stenosis lesions are often times more subtle and the radiology reports might not inspire a sense of seriousness. A bulging disc is extremely common, and can be mentally brushed off by accident. Be aware of this common mistake.
Each defendant here could point the finger at someone else and give an argument about why it wasn’t their fault. There’s plenty of blame to go around. But there was only one person who finally bothered to look at the entire situation and put it all together: the patient’s PCP. This illustrates the value of primary care, and how a generalist can help navigate disjointed, compartmentalized care.

I pulled 2 cases that I’ve published that have a very similar fact pattern:
patient can’t walk
lumbar spine MRI is negative
no one orders the thoracic MRI until it’s too late
Case 1: The lesion was a thoracic hematoma, missed by EM and neurology, after a negative lumbar MRI.
Case 2: The lesion was a thoracic epidural abscess, missed by EM, after a negative lumbar MRI.
Unfortunately, I have multiple more like this to publish over the next 1-2 years.
Join the email list to get all the best content!
Go to the ER and evaluate your post op patient when consulted by ER physician.
Or at least evaluate the patient as soon as feasible.
Stop the lazy practice of "admitting to hospitalists".
Hospitalists are excellent physicians in their own fields but they are not the surgeon who has operated on the patient. You may lose a few hours of sleep but you'll save yourself a lot of headache in the long run.
As a neurosurgeon, I have serious concerns about the spine surgeon who appears to have "brushed off" new bilateral lower extremity weakness. Did this person actually see and examine the patient? Or simply recommend steroids and follow-up sight unseen? Any decent neurologic exam would find abnormalities and the spine surgeon should have immediately recommended (and then followed up) the appropriate imaging (MRI T spine).