



A 58-year-old man went to an ophthalmologist with a bump on his left lower eyelid that was interfering with his vision.
He was a tenured professor of history at a prestigious university.
The patient had 20/30 vision in the right but could only detect hand motion in the left eye.
Pressures were normal in both eyes.
He was diagnosed with blepharitis and told to return for a recheck.
9 days later he came back for another appointment.
He was seen by an optometrist.
There was no improvement in the vision in his left eye.
He was advised to use antibiotic eye drops and use warm compresses.
His vision was still not improving, so he sought a second opinion.
A retinal detachment was diagnosed 15 days after the initial visit.
He was referred to a retina specialist and had surgery on the eye.
He did not regain any useful vision in the left eye.
Join thousands of doctors and attorneys on the email list.
The patient contacted a law firm and a lawsuit was filed against the first ophthalmologist and the optometrist he saw at the return visit.
The plaintiff’s expert witness opinion is shown here:
The plaintiff disclosed a second expert that specifically addressed the differences in management with a macula-on vs. macula-off retinal detachment.

The defense hired an ophthalmologist to defend the optometrist’s care at the second visit:

Become a better doctor by reviewing malpractice cases from multiple different specialties.
Paying subscribers get a new case every week and access to the entire archive.
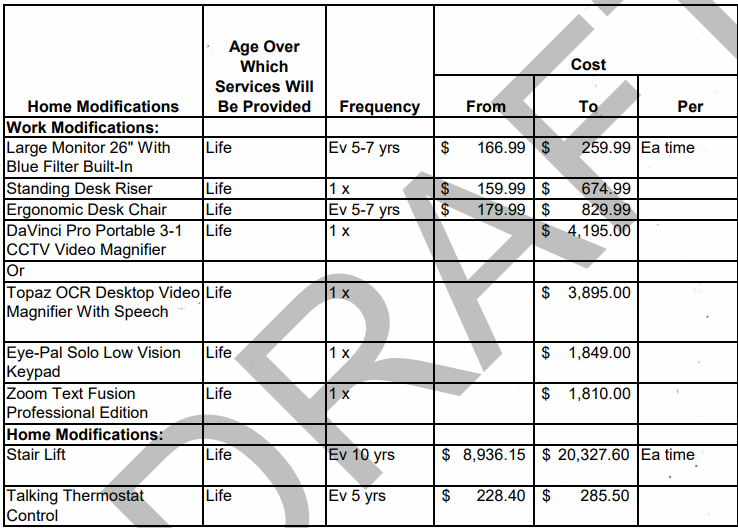
The plaintiff disclosed a report from a rehabilitation expert that included the cost of all of the possible accommodations that patient would need in the future.
This is an excerpt from the numerous pages of the report:
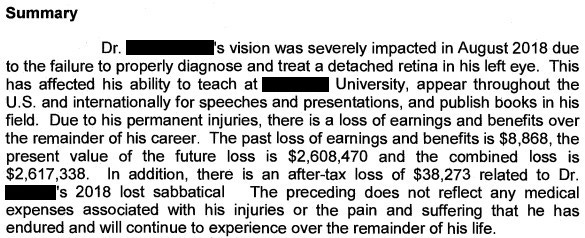
An economics expert was hired by the plaintiff to review his earnings, and estimate how much potential income was lost due to the patient’s early retirement.
All parties reached a confidential settlement before trial.
MedMalReviewer Analysis:
There are some good take-home points from this case, even if you never see patients with eye complaints. I’m guessing that the first ophthalmologist got “tricked” into focusing on the blepharitis because the patient perseverated on the bump on his eyelid. Sometimes the patient’s chief complaint is not actually the true chief complaint. We need to maintain respectful skepticism of a patient’s ability to accurately describe their problem. We also need to be mentally alert to the possibility of a previous misdiagnosis when seeing a patient for a follow-up appointment.
It’s very telling that the defense didn’t disclose any experts to defend the first ophthalmologist who missed the diagnosis. I’m not an ophthalmologist, but it seems quite rare that blepharitis would cause such severe loss of vision.
The accommodations claimed by the plaintiff seem a bit excessive. A $20,000 stair lift may be necessary for someone who was rendered paraplegic, but does monocular vision really prevent someone from walking up steps? It’s rare that these rehab/economic assessments are included in court documents so I found it very interesting to see what they try to claim.
Here are three other eye-related cases I’ve covered before that all involve an ophthalmologist getting sued:
I feel bad for this patient, and the miss does seem egregious, as blepharitis should not cause such bad vision loss. However, the estimates of lost income seem absurd. He really couldn’t continue to do his job as a professor due to losing vision in one eye? I had an attending when I did EM residency that was able to keep working as an ER doc even after he lost his eye in a golfing accident. He was still able to do LPs and everything.
Looks like a bad miss.