


Stroke After Warfarin Held for Hematuria
Case #235

An elderly man presented to the ED with hematuria.
He had a history of CKD, previous cerebellar strokes, anemia, hypertension, diabetes, and a prior kidney mass.
The workup included a UA that confirmed hematuria, creatinine was at baseline (2.28), and stable mild anemia.
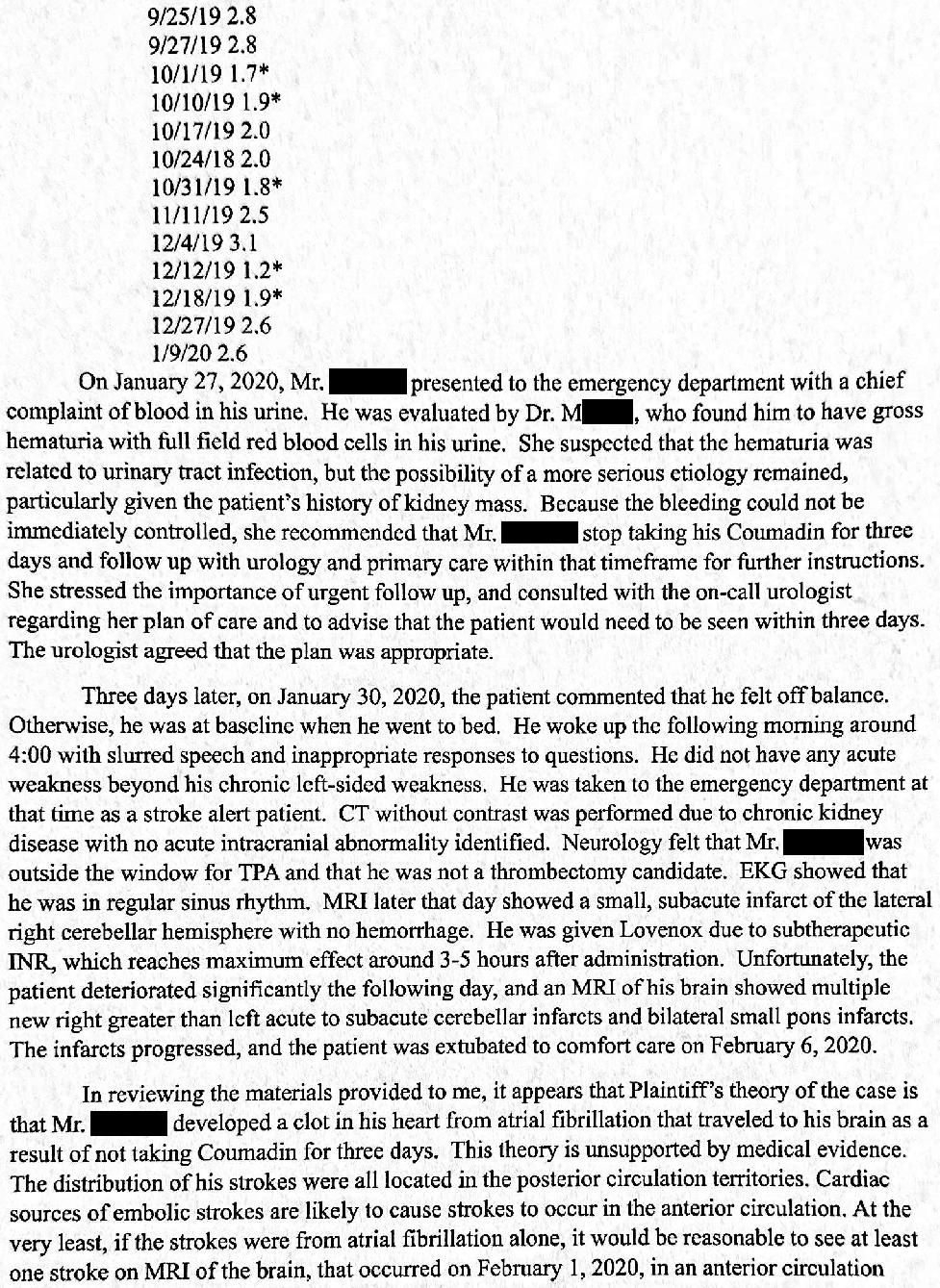
He was on warfarin for paroxysmal atrial fibrillation, and his INR was 2.15.
Given his normal vitals and no sign of any other complications, the ED physician felt the patient could be discharged home.
She spoke with the patient’s urologist, who agreed to see him in follow-up for further assessment of the source of the bleeding.
Cefuroxime was started for possible UTI due to having 10-20 WBCs on his UA.
The ED physician also advised the patient to stop taking his warfarin for 3 days.
The patient was told to call his PCP and urologist the next morning to help expedite his appointments. He was given their phone numbers on the discharge papers.
Unfortunately, the patient did not make any phone calls.
His PCP called 2 days later to set up an appointment, but the patient didn’t feel it was necessary and declined the offer.
4 days after the index visit, the patient woke up with left side weakness, facial droop, slurred speech, and vomiting.
He was taken to a different ED as a stroke alert.
CT head was unremarkable, but MRI showed a small subacute infarct in the right cerebellum.
No CTA was done due to his poor kidney function.
His INR was 1.2.
The patient was started on Lovenox and admitted.
Over the next 36 hours, the patient had slowly worsening mental status.
The hospitalist ordered several repeat head CTs that were all negative.
The radiologist recommended a CTA in multiple reports, which was not done due to the patient’s CKD.
Instead, an MRA was done which showed a left vertebral artery occlusion, bilateral cerebellar infarcts, and pons infarct.
The patient’s mental status declined further and he was intubated for airway protection.
The ICU doctor ordered a CTA head/neck, which showed obstruction of bilateral vertebral arteries and the basilar artery.
The case was reviewed by an interventional neurologist at another hospital but he was deemed to not be a candidate due to the fact that he had been declining for over 24 hours.
The patient’s family withdrew care and he died.
Become a better doctor. Join the email list.
2 years after he died, the family filed a lawsuit.
They sued the ED physician and the PCP.
The PCP was dropped shortly after it was filed, without a settlement.
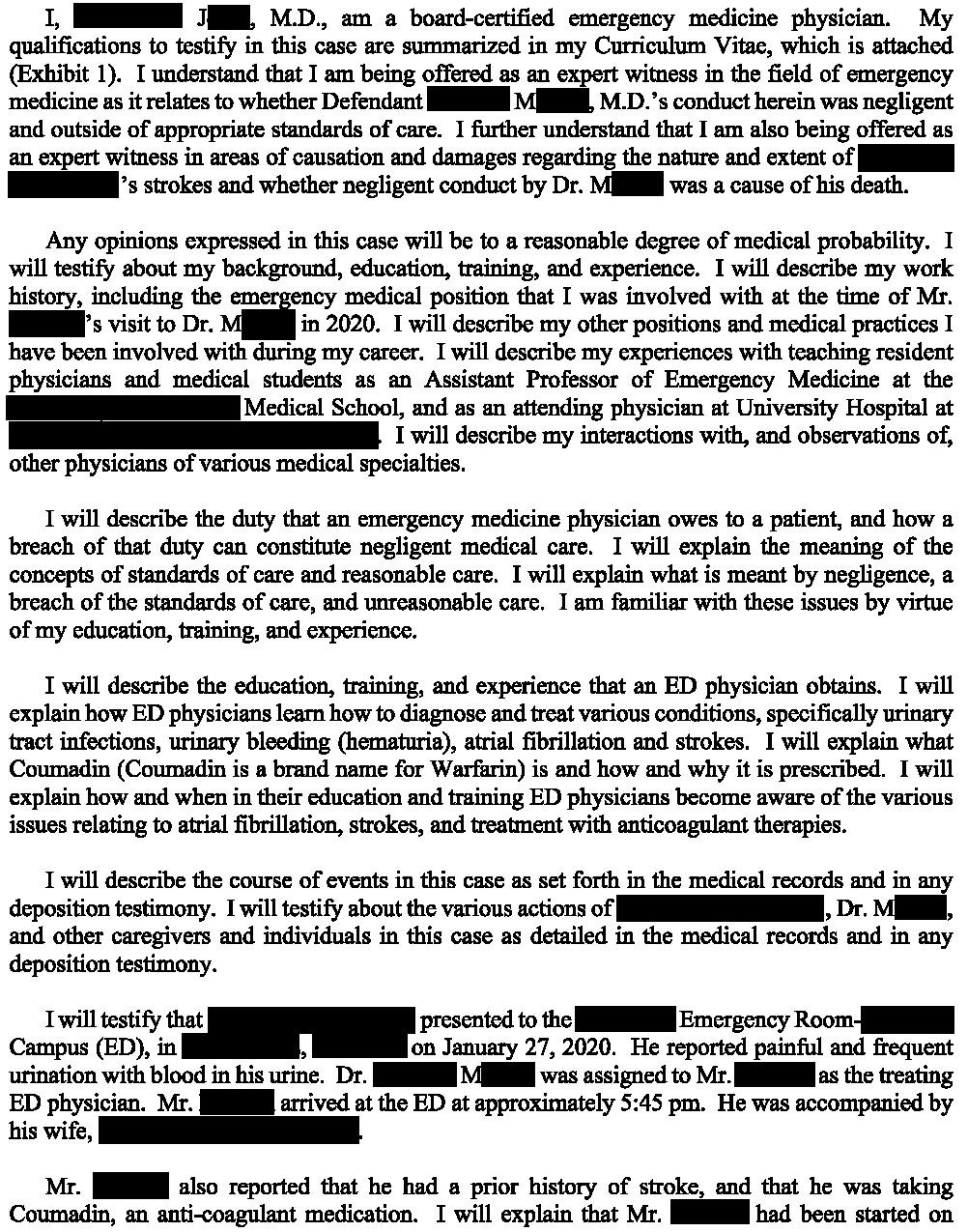
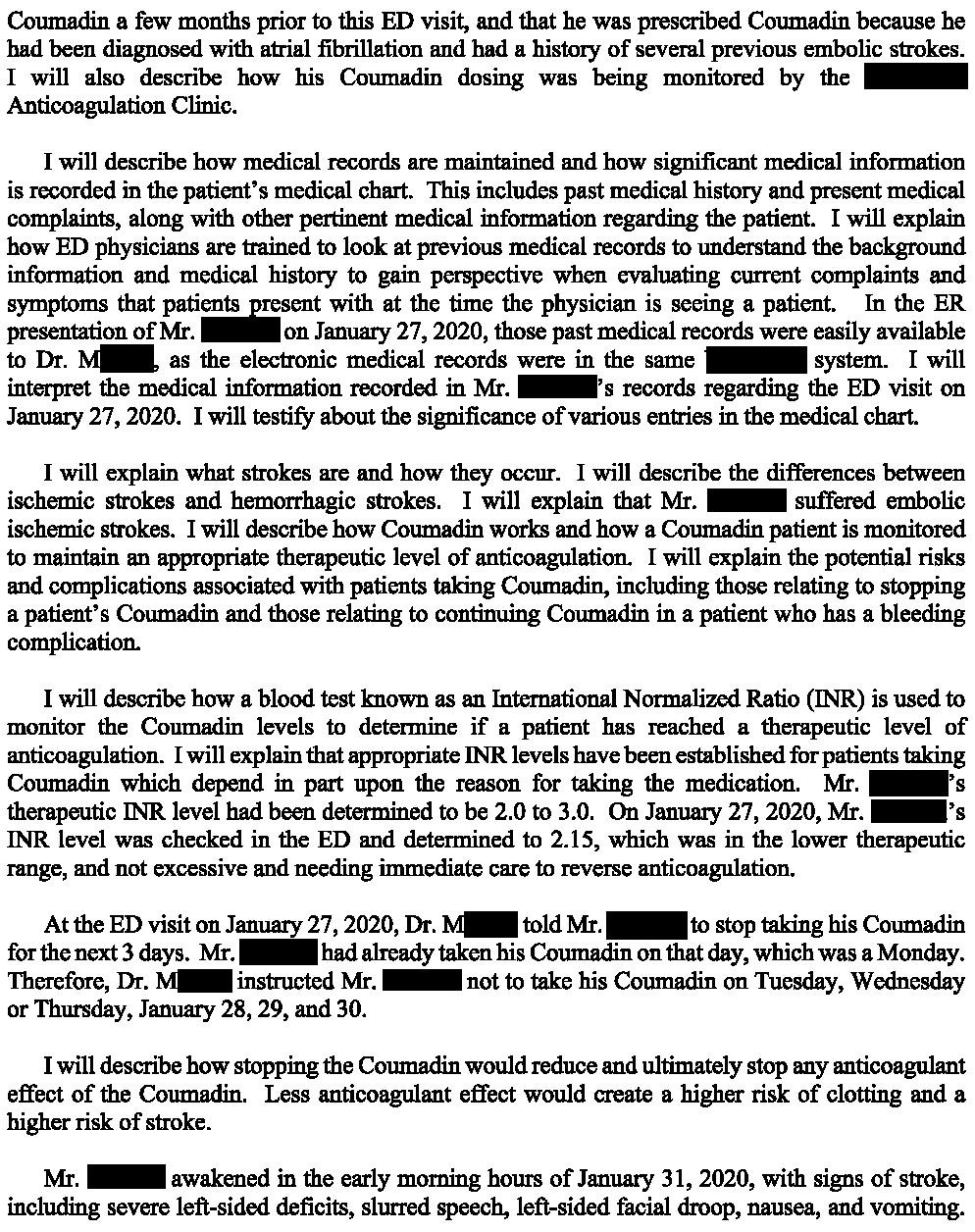
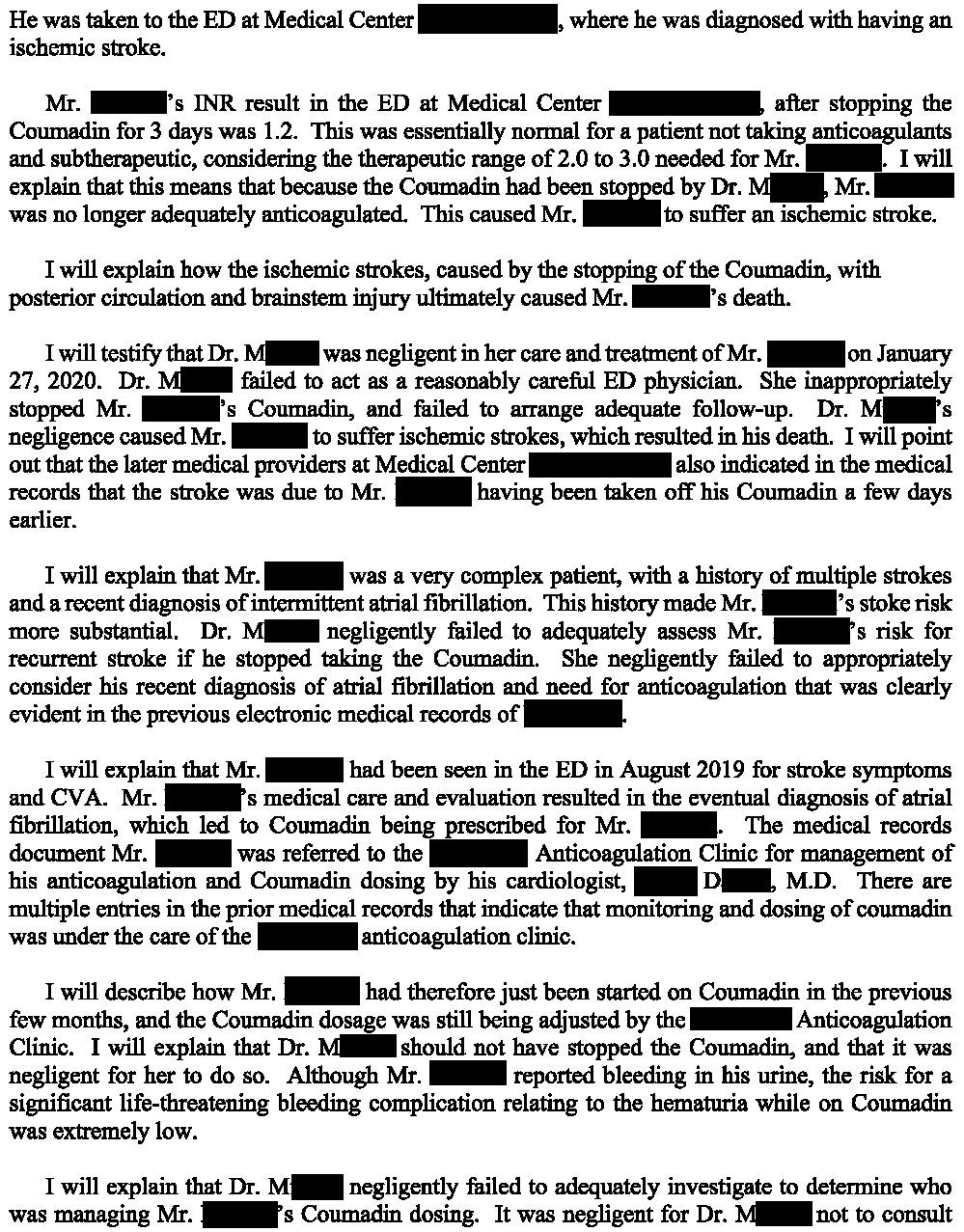
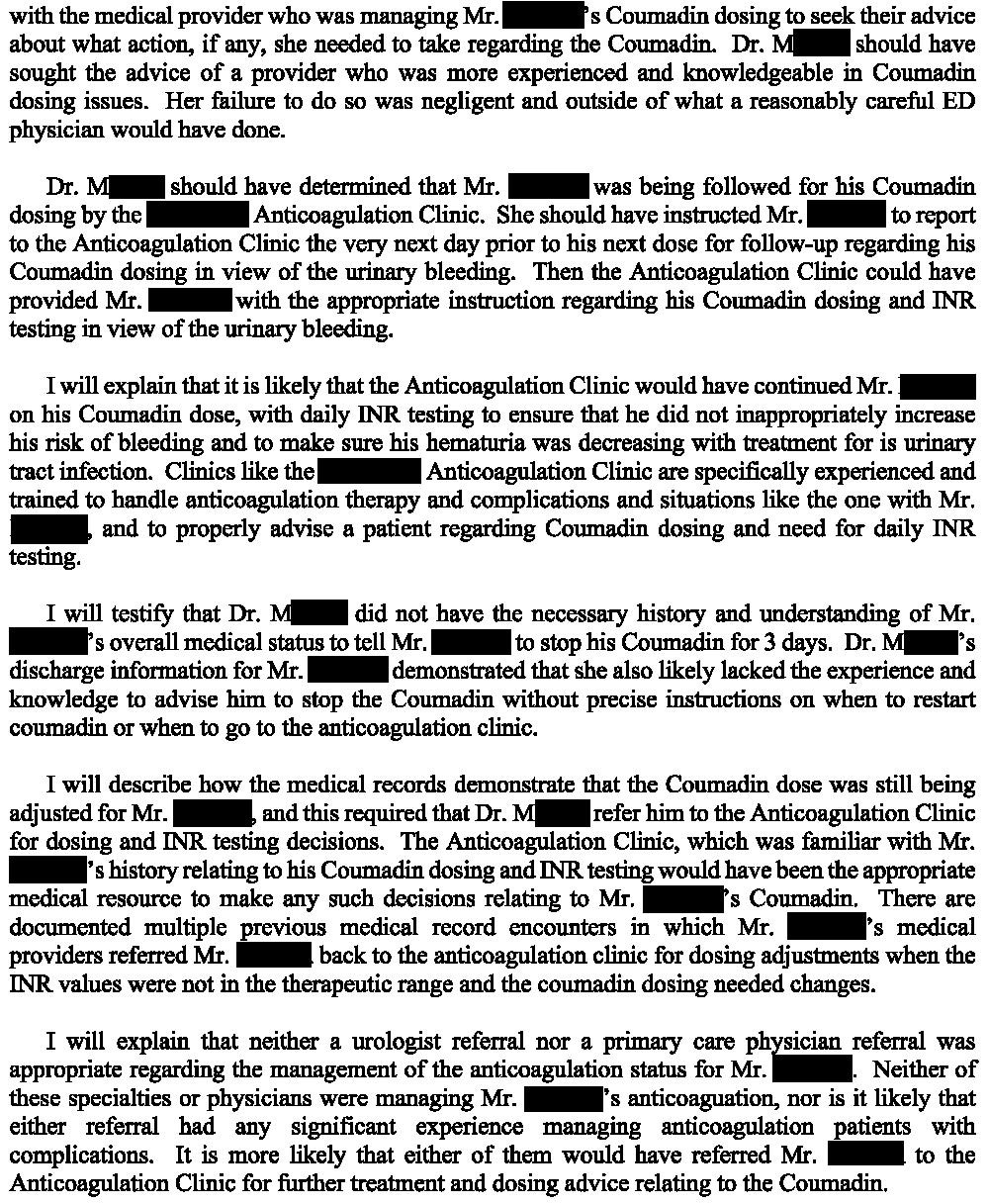
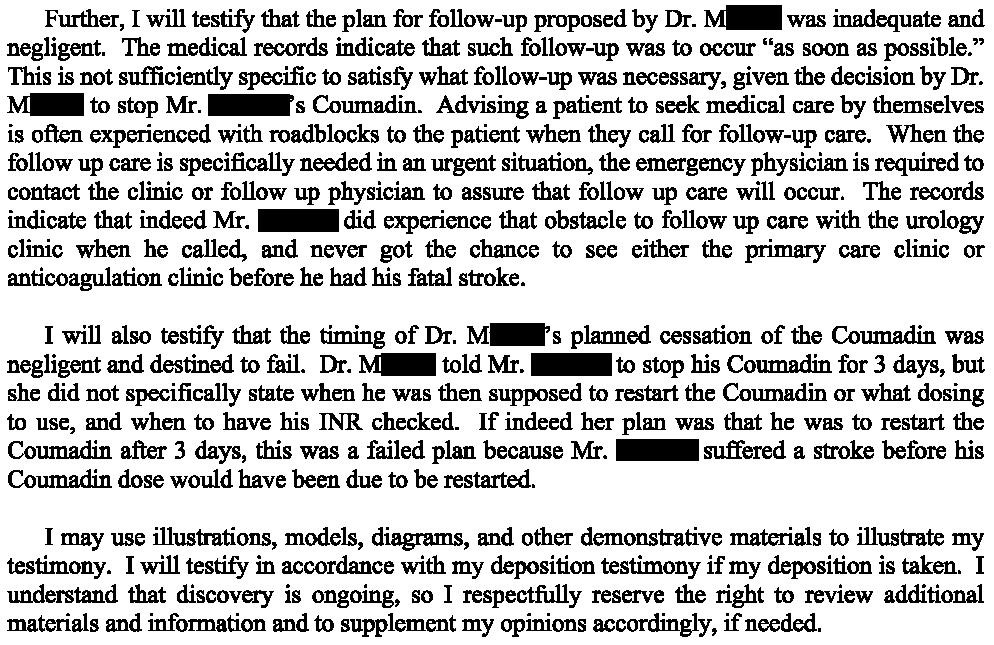
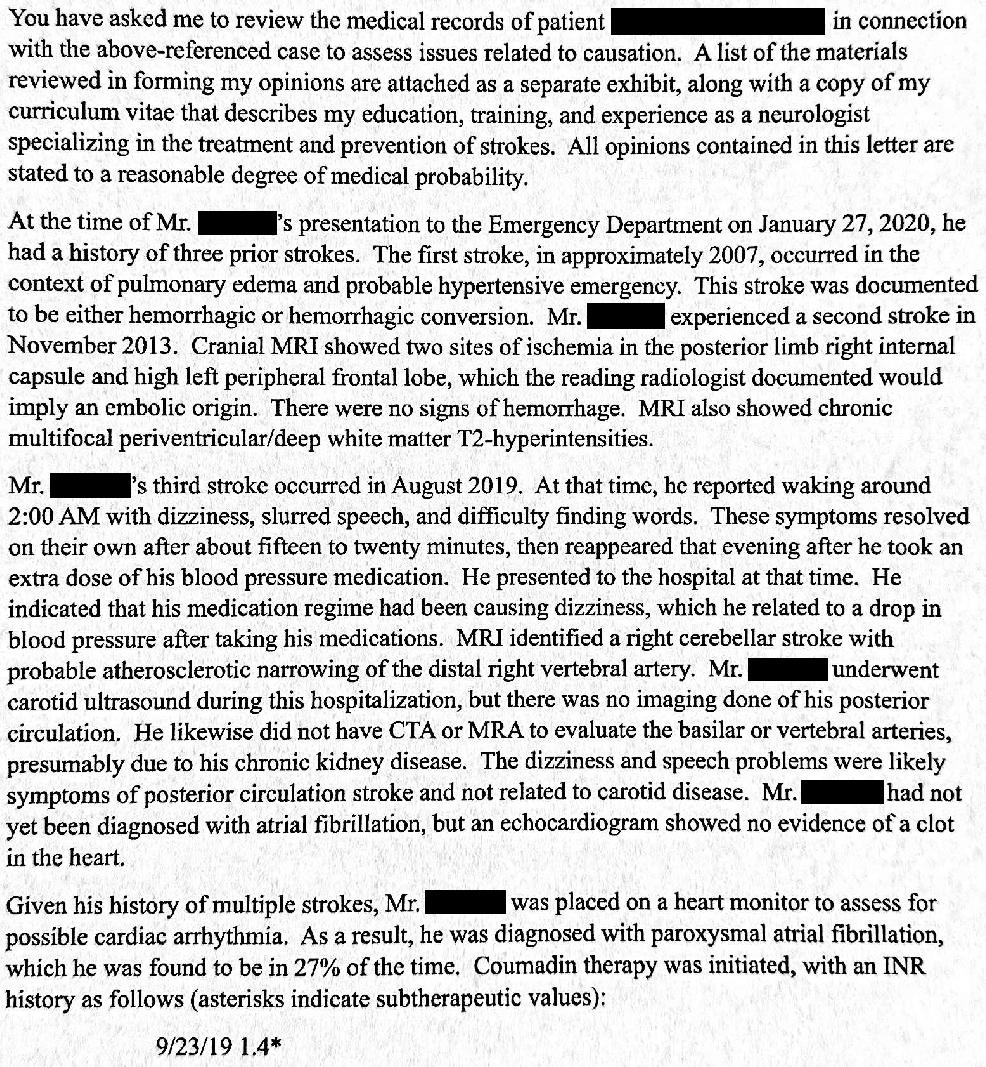
The plaintiff’s EM expert opinion is shown here:
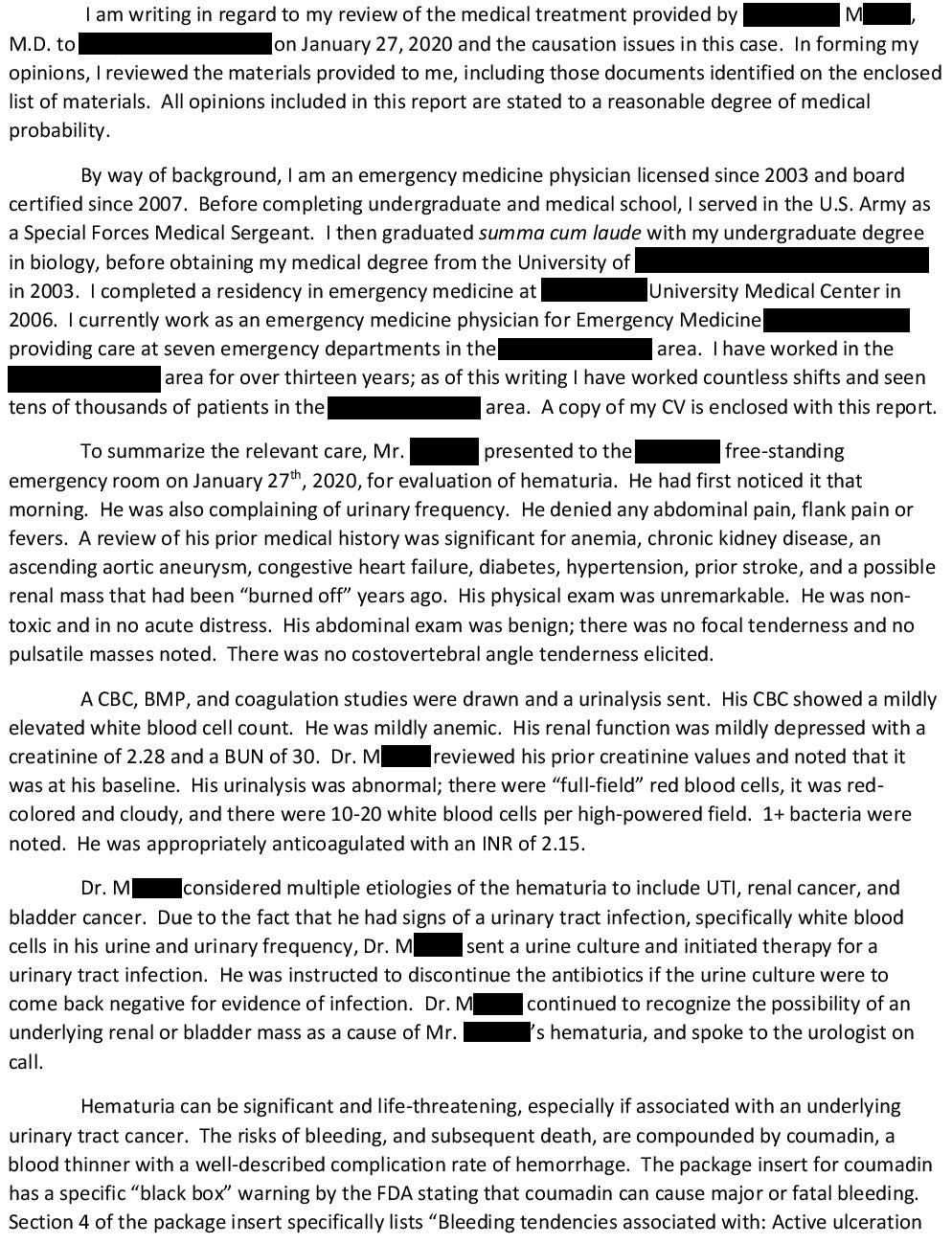
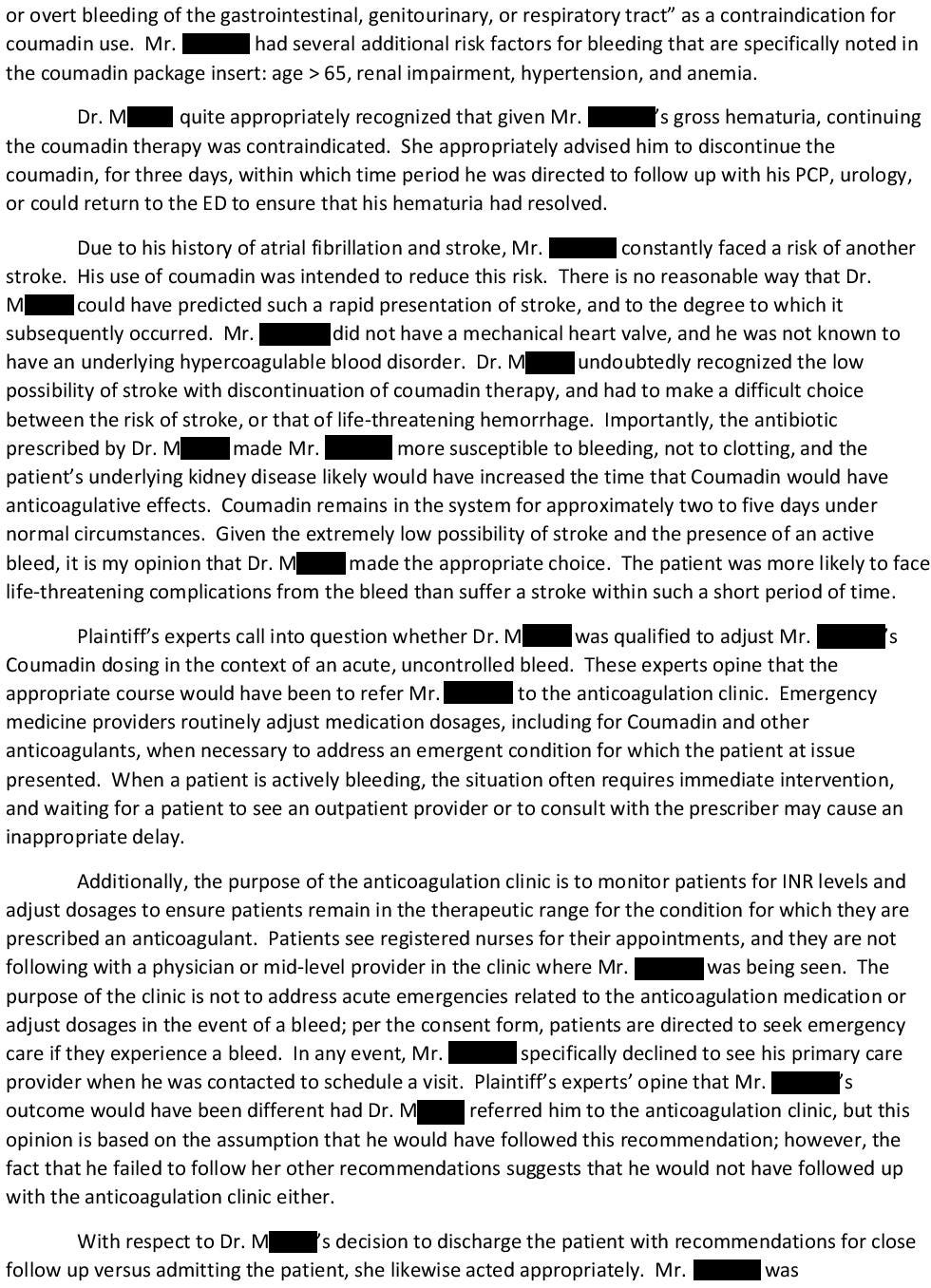
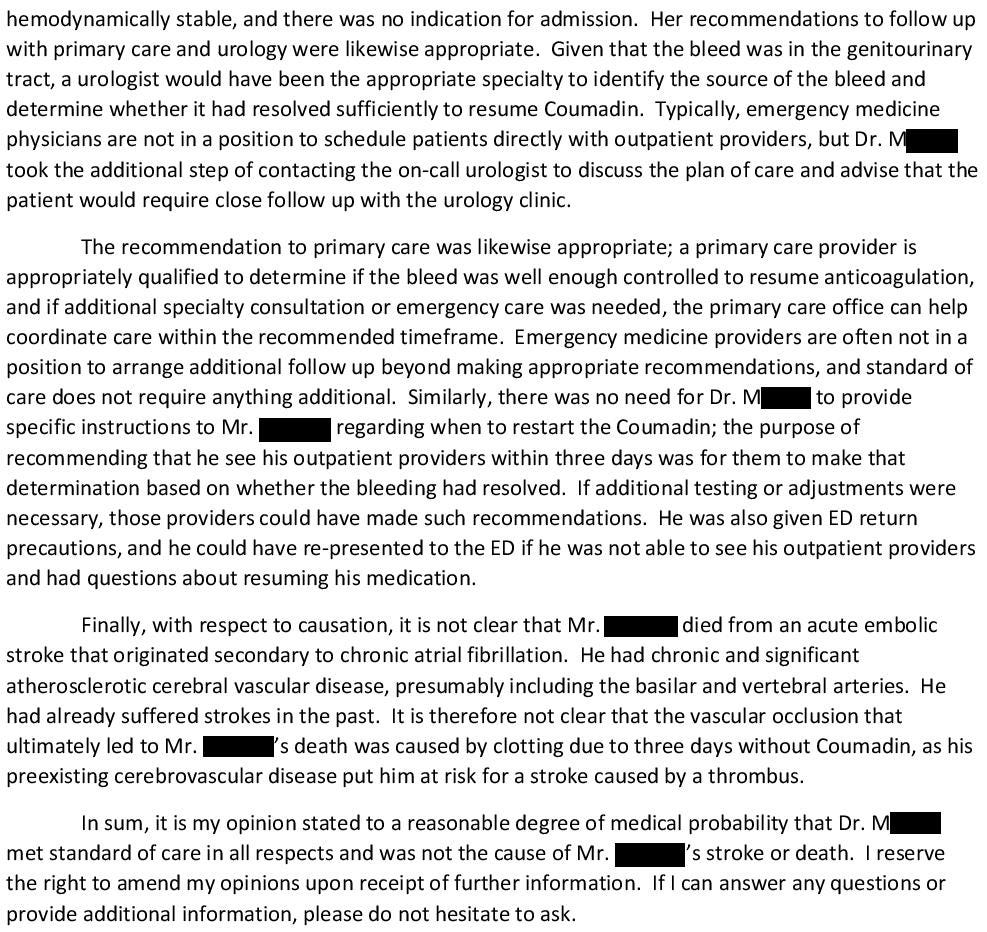
The defense EM opinion is shown here:
Subscribing will help you gain knowledge that can reduce the likelihood of being sued.
Subscribers get a new case every week and access to the entire archive.
The defense also hired a neurologist:
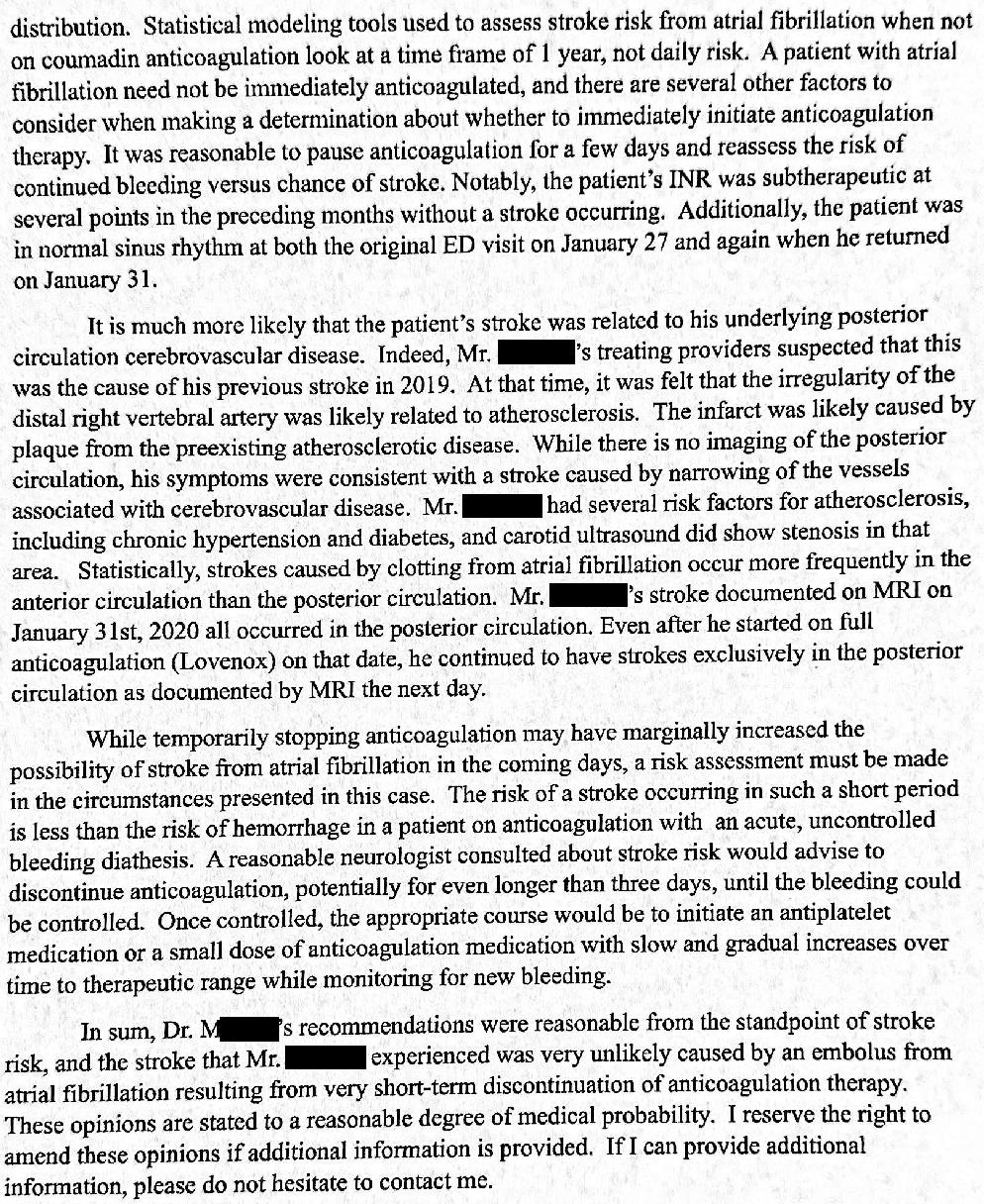
The ED physician refused to settle.
A few weeks prior to trial, the plaintiffs realized they were unlikely to win, and the lawsuit was dropped without a settlement.
MedMalReviewer Analysis:
In my opinion, the plaintiff’s EM expert made multiple dishonest claims. He claims that she should have consulted the anticoagulation clinic or provider who was managing the warfarin. EM doctors are perfectly capable of making this decision unilaterally, and the expert must have incredibly weak clinical skills (amounting to no more than a consult monkey) if he actually practices like this. He also claims that the follow-up plan was negligent. The EM doctor specifically advised the patient to call both PCP and urology offices (and gave him the phone numbers) the next day to set up follow-up. This is a perfectly reasonable approach, and able-bodied patients are responsible for arranging their own care. A patient’s contributory negligence (not following-up as explicitly instructed) is no reflection on the doctor’s care. It seems that the expert expects the EM physician to drive to the patient’s house, pick him up, and personally deliver him to the appointments. There are multiple other points in this expert’s opinion that are completely laughable, but I don’t have space to criticize them all here. This “expert” is a teaching faculty at a well-respected EM residency in the Mountain West. If the contents of this expert opinion are any reflection of the teaching there, it is very concerning. Either this expert is an incredibly bad EM doctor or (more likely), he wrote a dishonest opinion in exchange for cash. I’m not sure which is worse: to be stupid or to be unethical.
All decisions about anticoagulation have high medicolegal risk. Besides obstetrical birth injuries it’s the most common malpractice topic I see, so I’ll say it again for emphasis: All decisions about anticoagulation have high medicolegal risk! There’s not a single common error in these cases so it’s hard to draw any specific conclusions, but I think one key learning point is to have an aggressive and detailed conversation with patients about the inherent risks of starting or stopping anticoagulation. Some treatment decisions can be made quickly with only limited explanation, but this is not one of them. Patients usually sue because they suffered an unexpected bad outcome, so if you’ve warned them about the possibility of a specific bad outcome, it’s no longer unexpected and they’re less likely to sue. Ideally, include the patient’s family members in the discussion. They’re the ones who are more likely to sue you, so it’s arguably more important to talk to the family than the patient from a risk perspective. You should document these discussions in your note as best as possible. I don’t always take all of these steps in my own practice, but its the best way to protect yourself.
I’ve covered another case in which the type of ischemic stroke (embolic, atherothrombotic, watershed, etc…) was extremely important. In this case, a 53-year-old man had his anticoagulation stopped before a surgery, had hypotension during anesthesia, and woke up with a large stroke. The plaintiff blamed the surgeon for stopping warfarin, but the defense countered that it wasn’t embolic and that he had a watershed stroke that should not have been influenced by his anticoagulation status. The surgeon was not as fortunate as the ED doctor in this case, and lost at trial to the tune of $4,200,000. Sometimes plaintiffs win at trial even when all the evidence is against them.
Stroke After Anticoagulation Held for Procedure [Jury Verdict for Plaintiff]
·![Stroke After Anticoagulation Held for Procedure [Jury Verdict for Plaintiff]](https://substackcdn.com/image/fetch/$s_!aiw5!,w_1300,h_650,c_fill,f_auto,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Ff69fd2a5-9447-4211-bb0a-8909b1f5b023_940x708.png)
Editor’s note: This post is for paying subscribers, with a preview for free subscribers.
Giving contrast and getting a CTA probably would not have changed the outcome here, but I’m sick and tired of arguing about giving contrast to patients with elevated GFR/creatinine in the emergency setting. A patient’s very presence in the ED should justify the use of contrast ipso facto. Don’t let chronic kidney disease stop you from giving contrast if there’s a possible emergency. Don’t let an AKI stop you from giving contrast if there’s a possible emergency. No other clinician or tech should even be raising this issue with the bedside physician, let alone attempting to overrule their order.
![Stroke After Anticoagulation Held for Procedure [Jury Verdict for Plaintiff]](https://substackcdn.com/image/fetch/$s_!aiw5!,w_1300,h_650,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Ff69fd2a5-9447-4211-bb0a-8909b1f5b023_940x708.png)
The ED doctor actually called the urologist to make sure he’d be able to make an appointment. I agree with your point that patients need to take some responsibility in managing their own care. In terms of the CTA- these are routinely ordered in patients with suspected stroke and known kidney disease. In stroke alerts- we don’t even wait for creatinine to come back in most cases.
In regards to CT-A in setting of renal disease, i usually have a conversation with the pt and family and discuss risks of ESRD, and permanent dialysis as possiblities. It's rare but so is a stroke after stopping coumadin for a few days. That said, i really hate how doctors are held for bad outcomes, which we have absolutely no control over, unless we flippantly treat outside the standard of care. In this case, the ER doctor did what all other doctors would of done.