
Tardive Dyskinesia
Case #207

A 48-year-old woman presented to a psychiatrist (Dr. M) in May 2006.
She was diagnosed with depression, anxiety, and alcohol dependence.
Trazodone was prescribed to address difficulty sleeping.
At a follow-up appointment, she noted that trazadone was not helping.
Dr. M switched her to quetiapine (Seroquel) to see if it would help her sleep.
10 months later (April 2007), she had another follow-up appointment.
She had a developed a limp.
Dr. M referred her to an orthopedist and neurologist.
In August 2007, she had another follow-up appointment with Dr. M.
She was still having difficulty walking, and this time noted muscle spasms.
Dr. M decided to discontinue quetiapine.
She was seen at a movement disorder clinic, and told that she may have developed tardive dyskinesia from taking quetiapine.
Join thousands of doctors and attorneys on the email list.
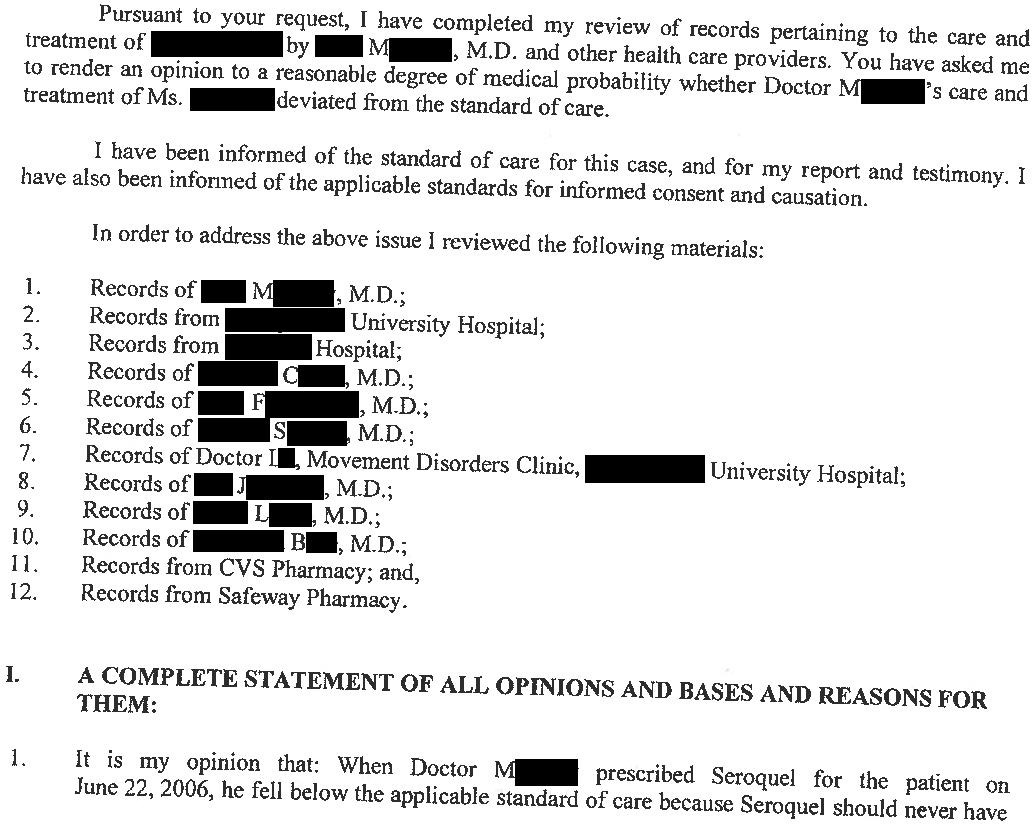
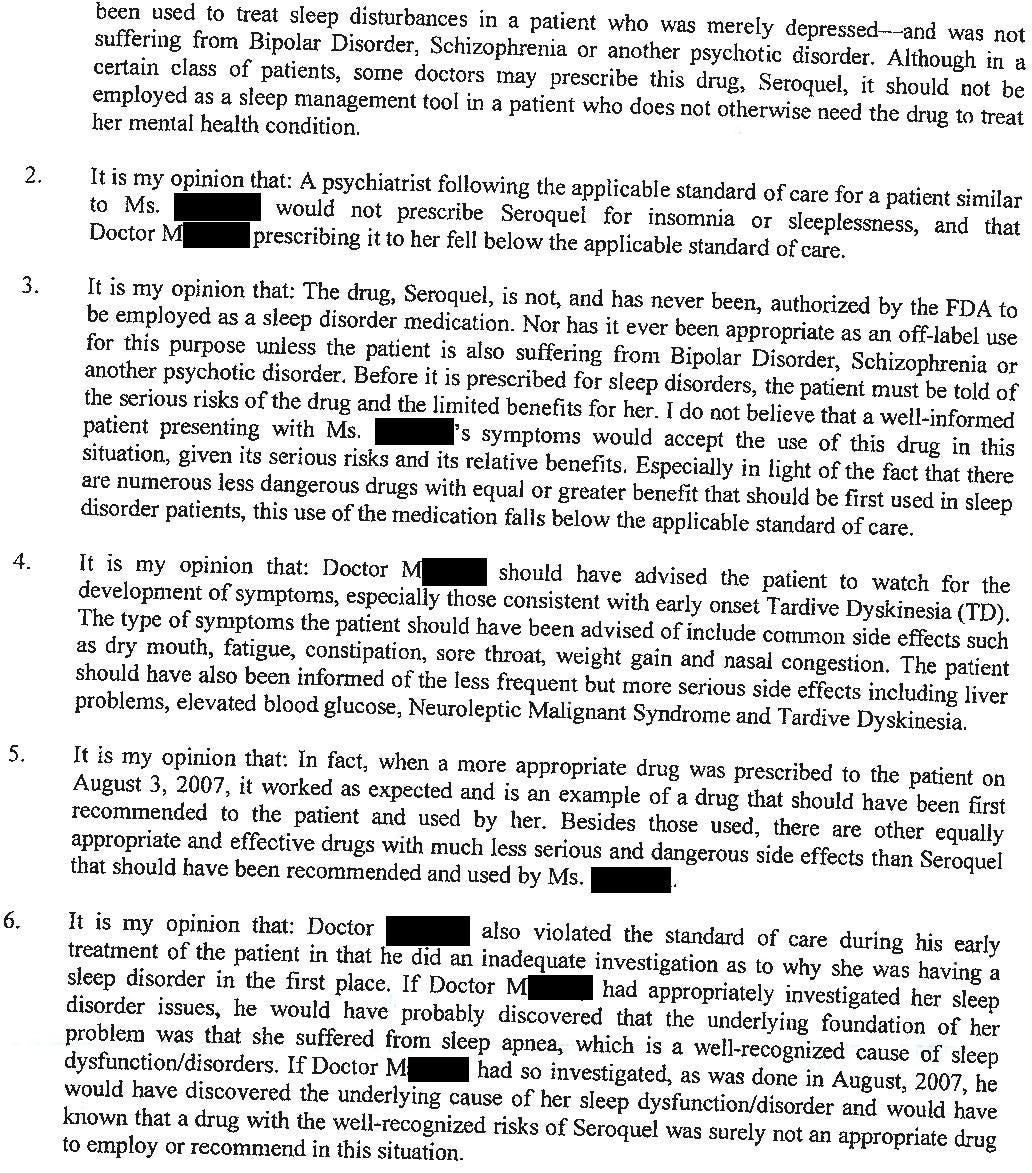
The patient filed a lawsuit against Dr. M, alleging that prescribing quetiapine for sleep was negligent, that he should have informed her of this risk, and should have tapered her off quetiapine much earlier.
The plaintiff’s expert report is shown here:

Become a better doctor by reviewing malpractice cases from numerous specialties.
Paying subscribers get a new case every week and access to the entire archive.
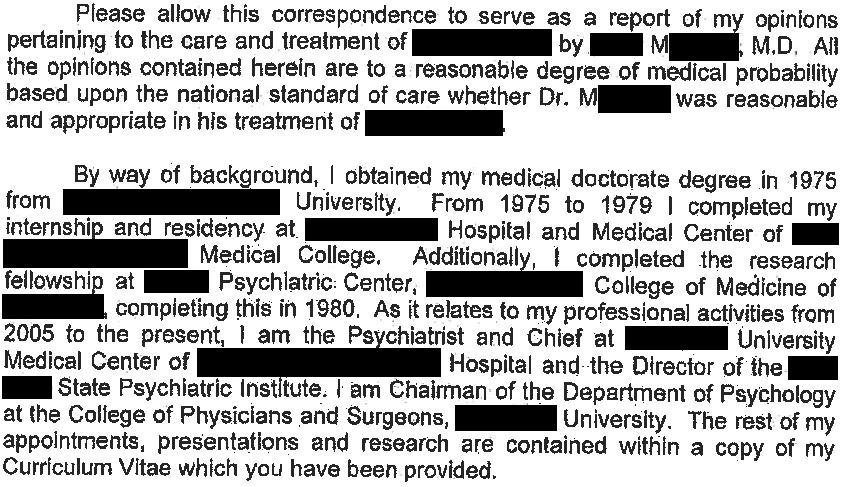
The defense hired their own expert witness:
Settlement negotiations were not successful, and the lawsuit went to trial.
The jury returned a verdict in favor of Dr. M.

MedMalReviewer Analysis:
The plaintiff did not make a very compelling case that the patient’s alleged tardive dyskinesia was caused by Seroquel. I reviewed this case with a consultation-liaison psychiatrist who noted several points:
Seroquel does not have significant D2 antagonism at the low doses used for sleep, and the patient was only on it for about a year. Higher doses of antipsychotics for longer periods of time have a much stronger association with tardive dyskinesia.
Limping would be a very unusual presentation of tardive dyskinesia. Abnormal movements of the face and tongue are much more common, and it doesn’t seem that the patient had these.
Use of Seroquel for sleep is very common and well within the standard of care.
Its always reassuring to see a jury reject highly questionable accusations of negligence and decide in favor of a physician. In general, juries are very favorable to physicians and decide in our favor in the large majority of cases that go to trial.
I agree wholeheartedly with the points raised by your C/L psych contact. Personally, I hesitate to use quetiapine just for insomnia (I think there are cleaner ways to get histamine blockade if that's the mechanism you're shooting for), but it is far from unusual especially if it can pull double-duty (e.g., as a mood stabilizer, antipsychotic, or antidepressant augment). Insofar as it's dosed for insomnia (usually 25-50 mg), its D2 affinity is negligible. It doesn't become a respectable antipsychotic until around 300 mg for most patients. And indeed, tardive dyskinesia to the extent that it occurs at all with quetiapine (probably the second-lowest chance after clozapine) would be very unusual to present with a limp, and not orofacial or upper extremity disturbances. When it does develop, it may transiently worsen after discontinuation of the neuroleptic, but should thereafter improve as the D2 receptors' sensitivity renormalizes.
And I'll just say as a psych hospital consultant myself, if quetiapine for insomnia constitutes malpractice, then half of the patients I see in the hospital should be contacting lawyers. Yes, it's "off-label." So is trazodone, at least for insomnia. Unless Dr. M. used a bombastic dose of the stuff or straight up lied about its side effect profile, it strikes me as very tough to carry a malpractice claim on an incidental (and very suspect) side effect alone. Glad to see the jury was of similar mind.
I agree with Dr.Skywalker. If the psychiatrist had lost this case, I would had to pull all my patients off of low-dose quetiapine for insomnia.