


Thoracic Back Pain Death [NP]
Case #56

A 52-year-old woman developed back pain in the thoracic region.
She presented to an ED.
She was assigned the lowest triage priority (ESI-5) and seen by a nurse practitioner.
The NP did not order any testing.
The patient was given steroids and muscle relaxers, and discharged.
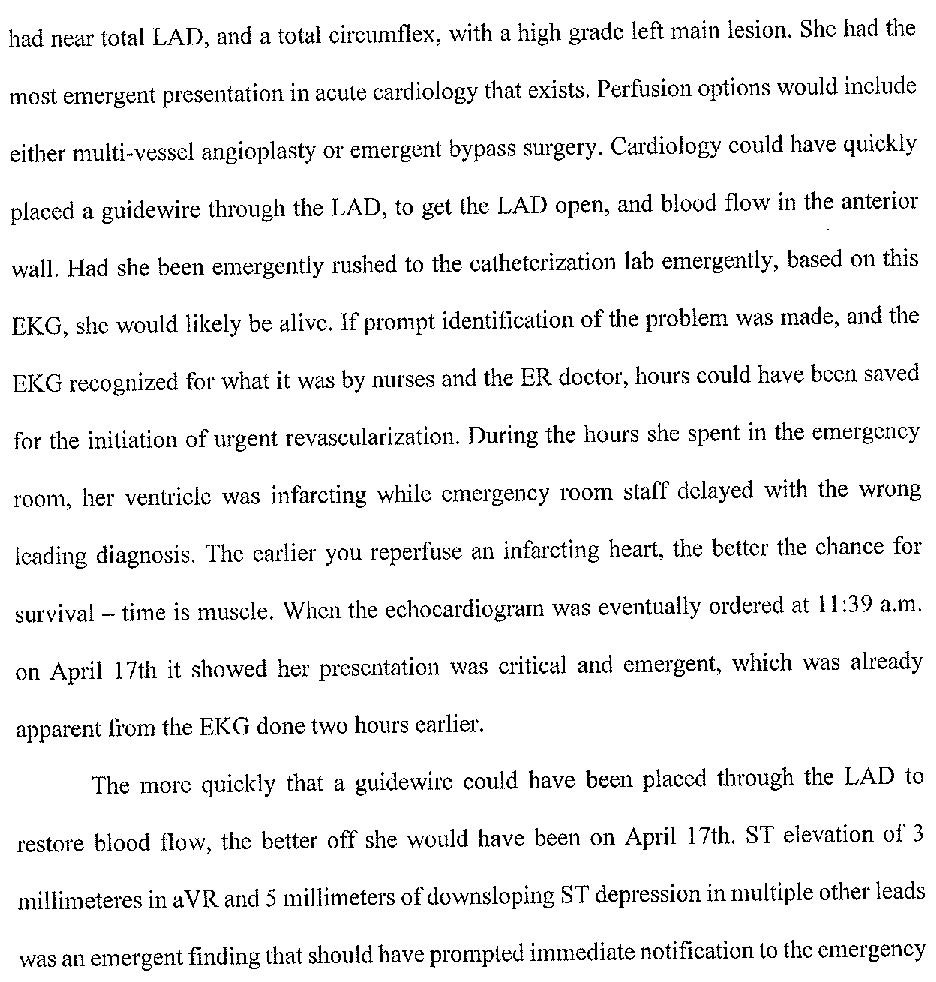
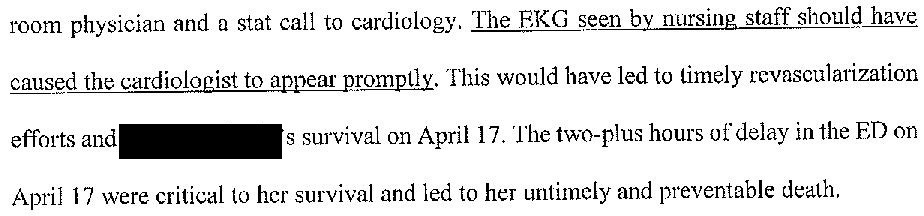
She returned to the ED several days later with a massive MI and died in the cath lab.
Become a better doctor by reading medical malpractice cases.
Paying subscribers get a new case every week and access to the entire archive.
The patient’s husband hired an attorney and a lawsuit was filed.
The EM expert witness wrote the following opinion:




An interventional cardiology expert was also hired.
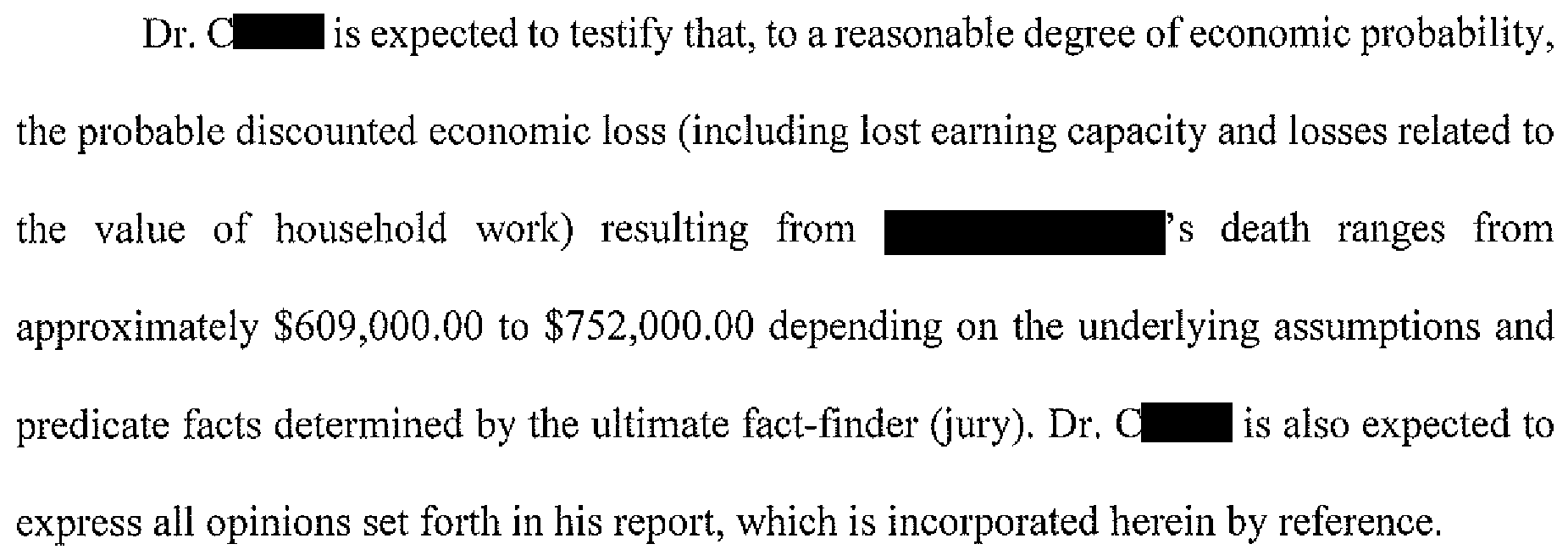
The plaintiff also disclosed an economics expert:
The two sides reached a confidential settlement.
Join thousands of doctors and attorneys on the email list.
MedMalReviewer Opinion:
When viewed from the EM expert’s perspective, this is a catastrophic missed diagnosis and it is difficult to find any perspective that would be favorable for the defendants. There are a few key learning points here:
Thoracic back pain warrants consideration of cardiac or pulmonary causes in addition to the typical spinal or MSK causes we usually think about.
The NP seems to have already mentally decided that this patient did not have anything serious based on the fact that she was seen in fast track.
The very existence of an area of the ED called “fast track” automatically introduces cognitive bias that these patients can be seen and discharged rapidly. Being self-aware of this bias helps prevent us from falling prey to it.Triage levels are useful only for deciding which patients need to be seen first. Once the patient is placed in a room, the clinician is wise to ignore the triage level and do their own independent assessment. Avoid anchoring to the (possibly incorrect) triage assessment. A healthy dose of skepticism about the assigned triage level is appropriate.
The cardiologist’s opinion offers a critical clue as to why the NP did not consider MI; the patient presented with back pain for a month that recently worsened. It would very unusual for an MI to cause a month of constant pain. This insight made me somewhat less critical of the NP.
The EM expert witness has numerous criticisms that are completely valid. Unfortunately, he oversteps at several points.
The expert rightly points out that the exam was lacking as there was no cardiac, pulmonary or neurologic exam. However, he makes numerous claims about standard physical exams that are not accurate. He claims that examining and documenting for a palpable heave, thrill, or thoracic bruits is part of a normal exam. He also states that assessment for “percussion note changes” would normally be done. This is a ridiculous claim. No one does an exam of that detail and it would not have aided in making the proper diagnosis. I would challenge this expert to prove that he does this on every patient with back pain.
The expert claims that a trapezius muscle spasm could not possibly occur in the thoracic or interscapular region. Any anatomy textbook plainly shows the trapezius extending into this area. He has no proof to back up his claim.
Agree on the two areas the expert overstepped, he really seems to be unable to help himself and is laying it on really thick.
97/40 in a patient in pain would catch my eye. It should be rechecked and discussed in the MDM. It might be as simple as "BP is low normal, lower than I would expect w her discomfort but she takes beta-blockers and the BP today is similar to the BPs recorded on her last two visits."
ACS is possible, but PE and dissection would also be high on my differential.
I've always thought of thoracic back pain as a trap. The differential diagnosis is broad, and reflexively concluding MSK cause is risky, as this case clearly shows. I can "reproduce" trapezius muscle tenderness, just as I can reproduce costochondral joint tenderness, but that doesn't mean I'm diagnosing costochondritis in everyone I see with chest pain. Not even close.
IMO, discharging a pt in 6-10 minutes is just plain bad practice. the NP clearly didn't adequately assess the patient. I'm not saying that no diagnostics were needed, but the whole chart is cringeworthy. I've reviewed plenty of these in M&M-poor documentation and shoddy care in the setting of a patient with soft vitals, high pain scale, and a complaint that suggests the need for more than a cursory evaluation.
Let's also point out that template charting and EMRs make this so much worse. you can make a chart look like you did a thorough assessment when in reality the opposite happened.