


Unrepaired Vaginal Laceration
Case #263

Friendly reminder - its the 5th Anniversary Sale!
Annual plans are 20% off and CME subscriptions are discounted to $395.
A young woman presented to her OBGYN after a positive home pregnancy test.
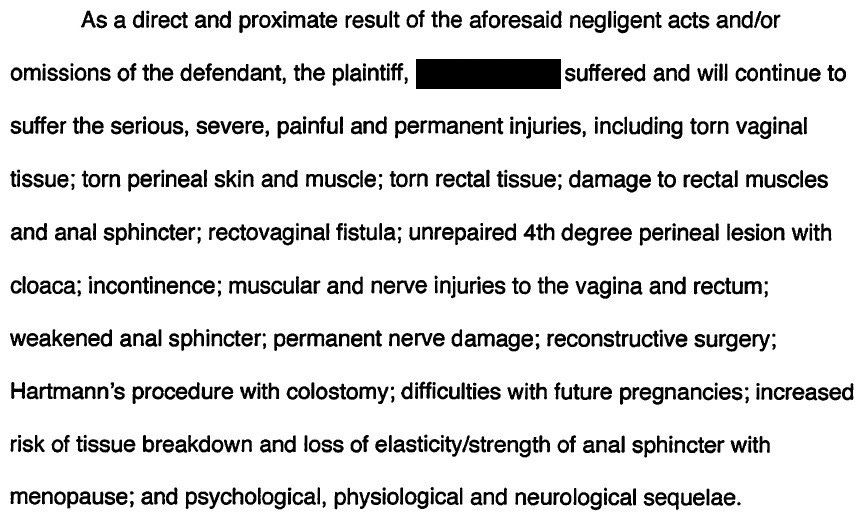
The pregnancy would ultimately culminate in a complicated delivery that would result in the death of her baby at 34 days old, and leave her with an unrepaired 4th degree perineal laceration.
The events are described here by the plaintiff.

Reviews from paying subscribers:
"As a Medical Director, and expert witness myself, I appreciate your perspective and analysis of these cases. Sharing them with my providers should help them avoid common pitfalls and increase their med mal awareness as well." - Dr. S
"As a wise man once said ‘always learn from your mistakes, but it is even wiser to learn from the mistakes of others.’ I support your work to learn about how to provide better medical care from the care others have provided.” - Dr. L
"Important and impactful case reviews -- excellent risk management education" - Dr. L
When the mother was transferred, both the doctors and nurses at each institution had a phone call to discuss the transfer.
The 4th degree laceration was not discussed in either of these conversations.
On arrival, nobody at the receiving hospital examined the perineum during the first few days.
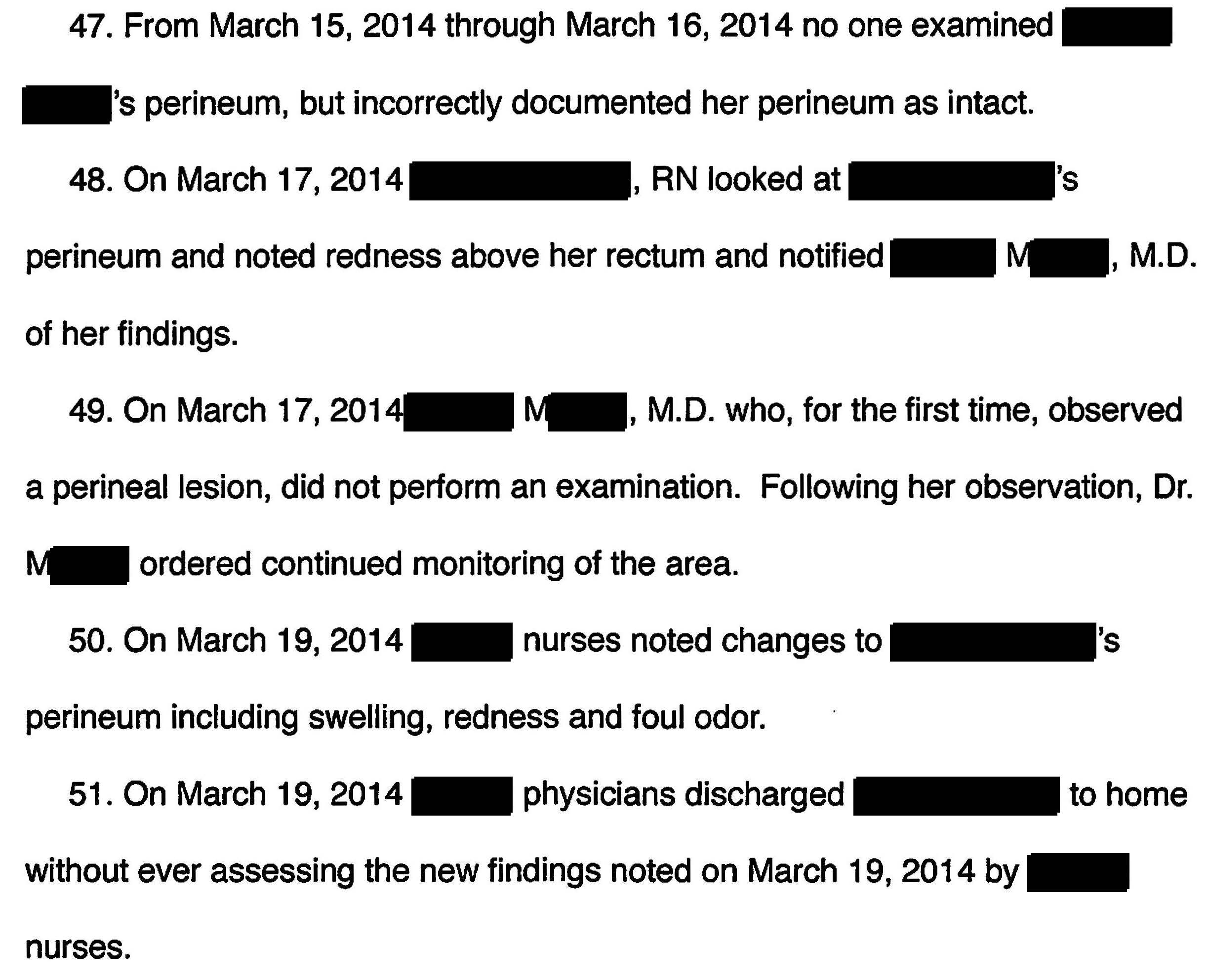
The 4th degree laceration was eventually diagnosed, but the patient was left with permanent debility.
A lawsuit was filed against all of the OBGYNs involved, multiple nurses, and both hospitals.
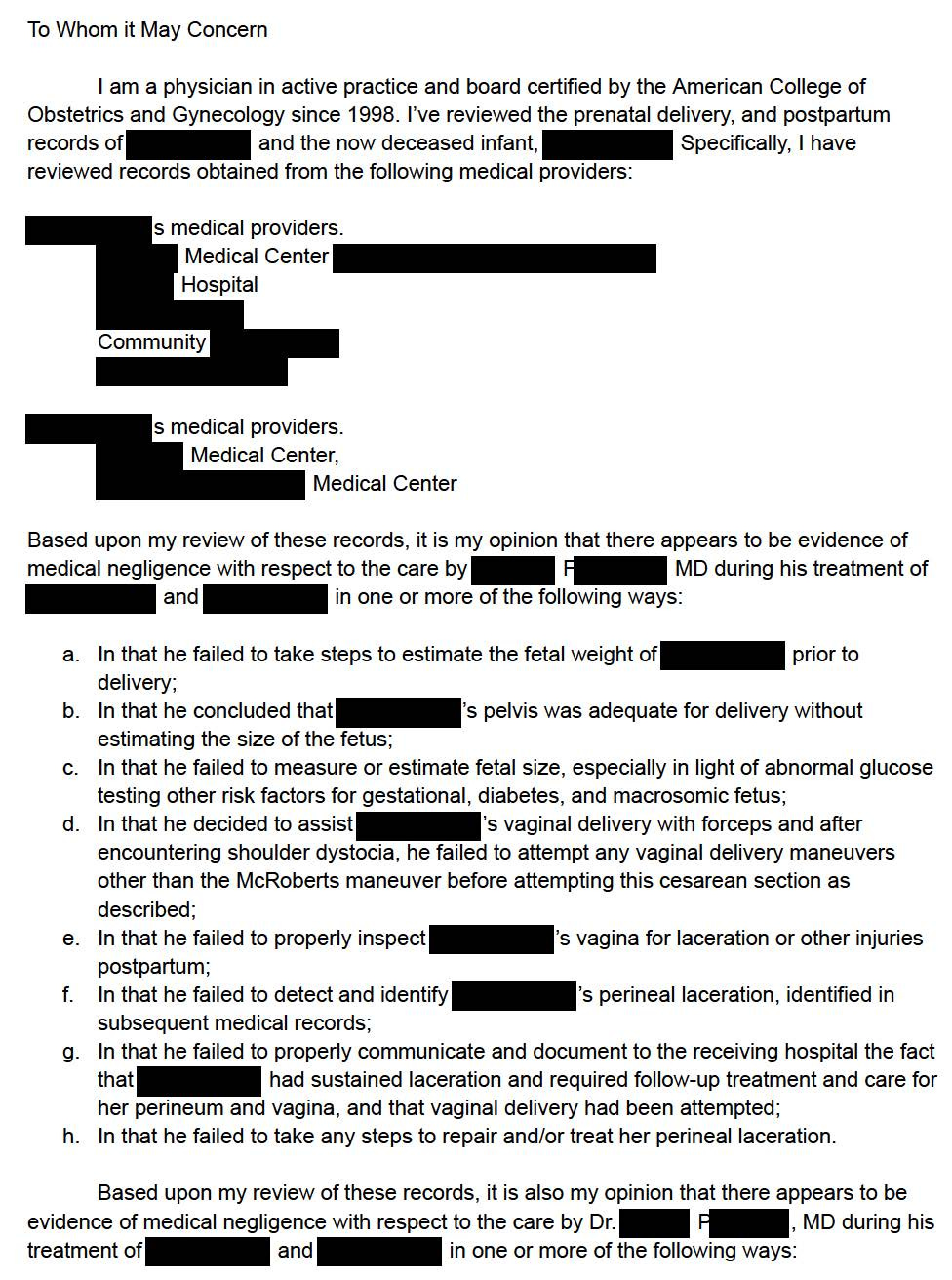
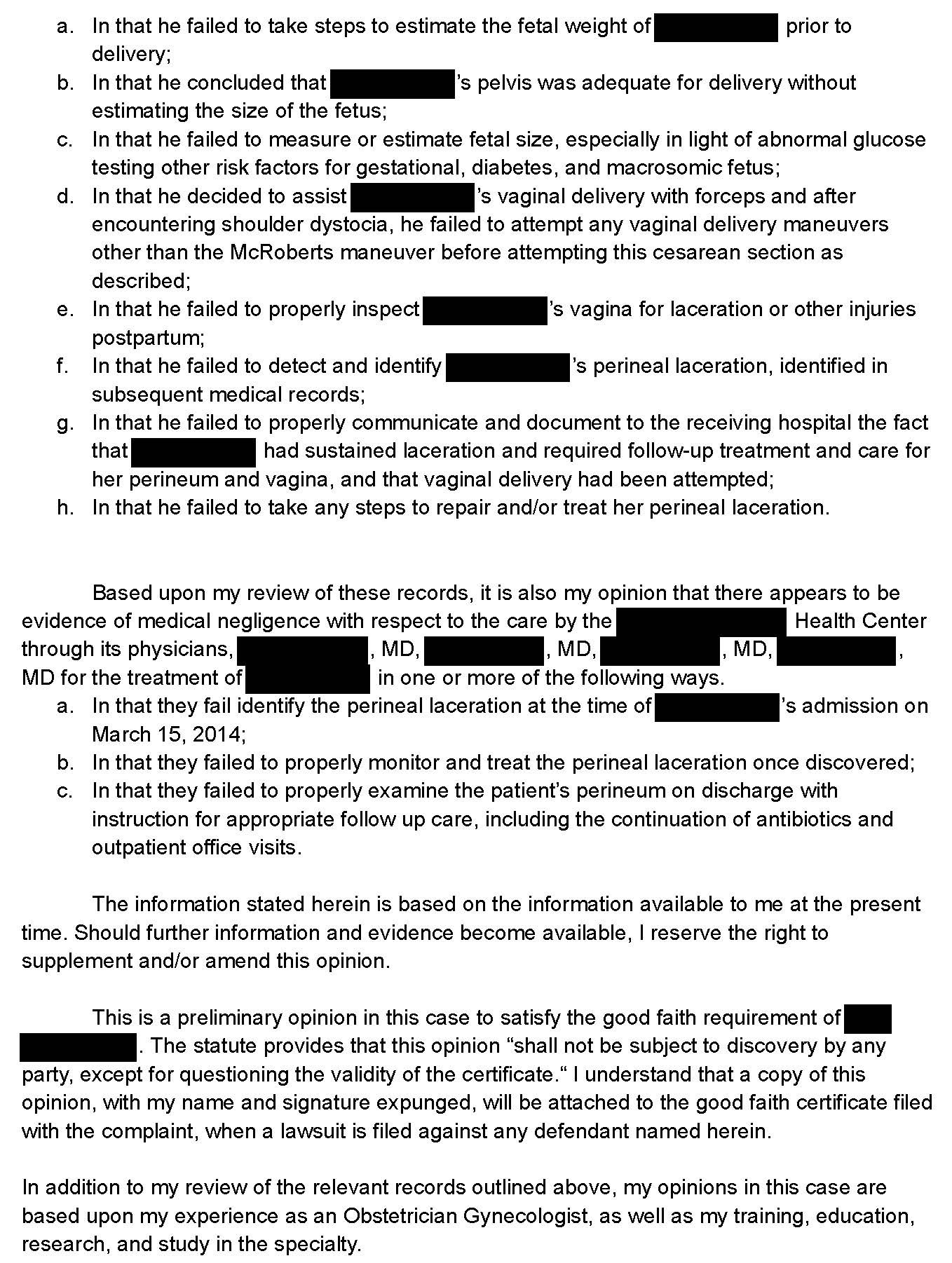
The OBGYN expert witness opinion is shown here:
The defense for the receiving hospital and OBGYNs hired an expert witness.
This expert testified that it was within the standard of care for them to rely on the information that they were given by the sending hospital, which did not mention any perineal injuries.
A confidential settlement was reached with all parties and the lawsuit was withdrawn.
I only run the anniversary once per year, now is your chance to lock in a discount!
Join thousands of doctors and attorneys.
MedMalReviewer Analysis:
It’s not clear to me if there was any medical reason that the mother needed to be transferred, or if she was simply sent so that she would be in the same hospital as the baby. Assuming the mother was stable and only needed routine post-partum care, it seems to me that the original OBGYN should have repaired her laceration. I could understand not repairing it if the patient was critically ill and there were other more urgent tasks that the physician needed to do, or if it was a stat critical care transport, but it does not appear this was the case.
My best guess is that the original OBGYN was so distracted by the shoulder dystocia, emergency C-section, and subsequent neonatal code that he forget to check her perineum. There were many distractions, but a well-trained physician should be able to navigate a stressful scenario without missing basic steps.
This case is a cautionary tale about accepting patients from the infamous “outside hospital”. When patients arrive, it’s important to thoroughly review all the basic steps of their care. Making assumptions can lead to missed issues like this. Even good doctors are susceptible to these mistakes from time to time.