


Woman's Abdominal Pain Misdiagnosed as Ovarian Cyst
Case #167

A 27-year-old woman presented to the ED with abdominal pain that she described as “central”.
She had undergone a cholecystectomy 5 weeks earlier.
Labs were normal, including the WBC count.
A CT scan noted normal post-operative findings, and a right-side ovarian cyst.
She was discharged with pain medication.
The next day she was still having severe pain (now in her right lower abdominal area), so she went to a different ED.
She explained that she was having severe pain from an ovarian cyst, and had a CT scan the day prior.
The ED physician ordered an ultrasound, confirming a ruptured right-side ovarian cyst.
Labs showed a normal WBC count with 36% bands.
She was given pain medication and discharged.
2 days later she returned to the ED with worsening pain and fever.
A CT scan showed ruptured appendicitis.
Her hospital course was long and arduous.
She went into septic shock, developed a DVT and PE, and had a cardiac arrest but was resuscitated with a good neurologic outcome.
The patient contacted a law firm.
They sued the radiologist from the first ED visit for missing a dilated appendix that contained multiple appendicoliths.
They sued the ER doctor from the 2nd visit for not ordering a CT scan and missing the diagnosis.
Both hospitals were also named as defendants.
Join thousands of physicians on the email list.
Paid options available for those who want to improve their practice through reviewing additional cases.
The plaintiffs hired a radiologist to review the case:

The plaintiff’s EM expert witness opinion is shown here:
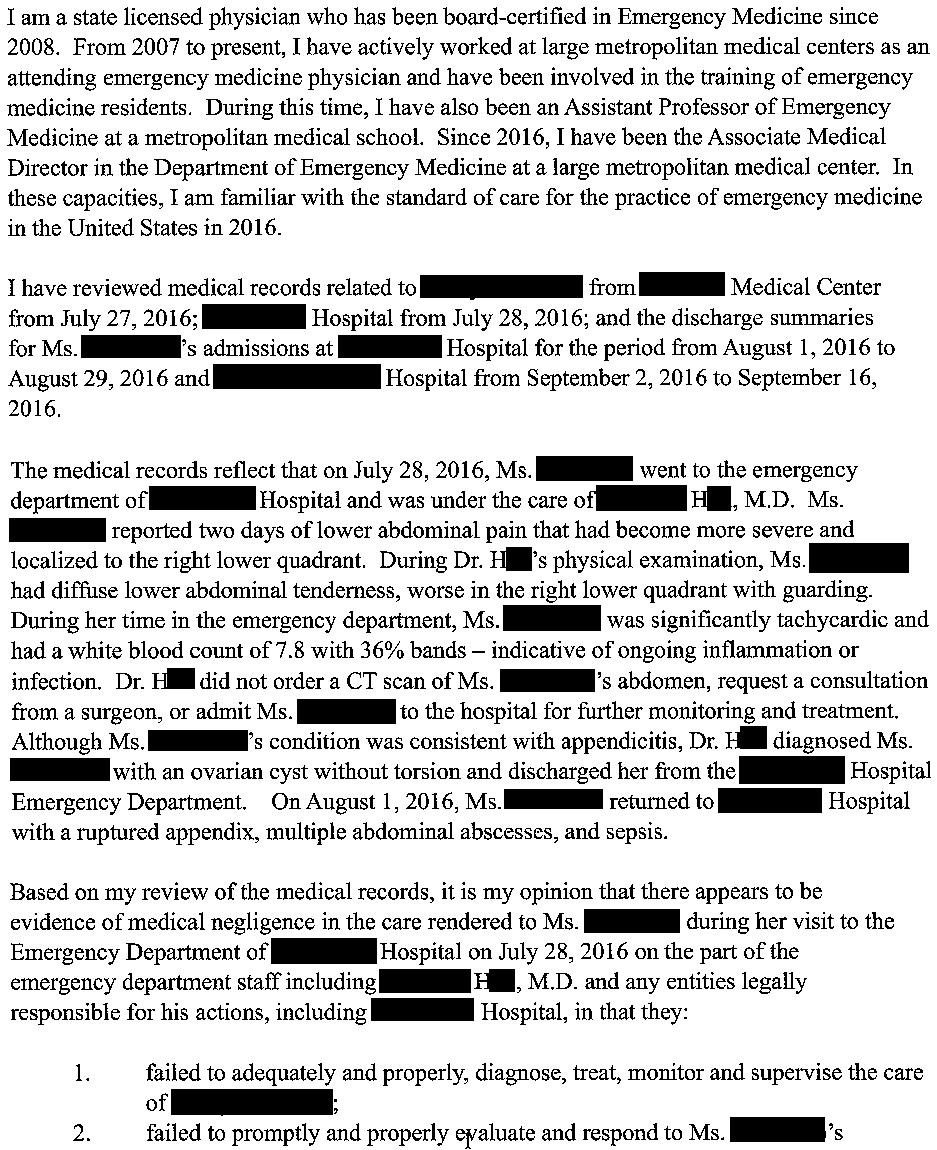
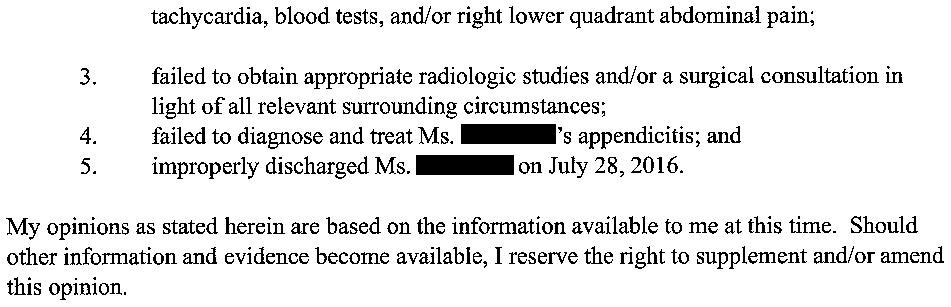
They offered to settle the case with both physicians and their respective hospitals:

The patient’s friends organized a fundraiser for her, raising $4,070.
The 2 sides have been unable to negotiate a settlement thus far.
The lawsuit is ongoing.
Subscribe to the newsletter to get updates on this lawsuit:
MedMalReviewer Analysis:
There were numerous factors working against the ED physician at the 2nd visit. This occurred at a different hospital, so he did not have any information about her workup 2 days earlier. The ovarian cyst was probably physiologic, but the fact that it was on the right side provided a possible explanation for her pain. There’s a good chance the doctor was told “I have pain from an ovarian cyst”, which accidentally caused diagnostic anchoring from the very beginning. When a patient tells you they have a diagnosis, some respectful skepticism may save them from a catastrophic outcome.
Bounceback ED visits must be handled with care. It may be the final opportunity to catch a subtle emergency or missed diagnosis before disaster strikes. Escalating the workup is sometimes indicated, but sometimes simply repeating the tests done previously can be helpful. Ordering another CT just 2 days later could be misconstrued as wasteful and causing unnecessary radiation exposure, but would have prevented this outcome.
To his credit, it appears the physician made an attempt to investigate further. He ordered an ultrasound to confirm the reported diagnosis and to rule out torsion. I think he has a valid argument that his care was reasonable and many other physicians would have done the exact same thing. However, I’m not sure I’d trust 12 random citizens to successfully parse the details.
In my opinion, the bulk of the liability falls on the radiologist for missing the appendicitis. The plaintiff describes a dilated appendix with multiple appendicoliths, which does not seem subtle. All of the other criticisms are downstream from this miss.
For the new ED physicians who will be starting their first attending jobs over the next few weeks, I wrote an article about how to orient yourself to a new job.
Here’s the link, let me know what you think!
This is why I scan. The risk of me missing something is more to me than the risk of them getting cancer…
This is probably one of my worst nightmares. I've experienced this diagnostic anchoring bias before, but I always try to ask the patient to describe any different symptoms compared to their recent/last ED visit. Without physically seeing this patient, I don't know if I would have repeated a CT scan two days later. I'd be interested in her SIRS criteria, just to see how the bandemia played out.