


Dead Child After Cancer Misdiagnosis [Case Update]

I originally published this case almost 3 years ago.
An 11-year-old boy was found to have a lesion in his cervical spine.
The diagnosis came down to osteoblastoma (good prognosis) vs. osteosarcoma (poor prognosis).
Multiple doctors reviewed the case and imaging, still without certainty.
A pediatric neurosurgeon took the patient to the OR, where frozen section slides were suggestive of osteoblastoma.
The neurosurgeon did a limited local resection (appropriate for osteoblastoma) as opposed to stopping to allow time for neoadjuvant chemotherapy followed later by radical total resection (necessary for osteosarcoma).
The permanent sections were more suggestive of osteoblastoma than osteosarcoma, so the team initially felt they made the correct decision.
Unfortunately, the cancer turned out to be osteosarcoma.
Autografted tissue used during the surgery resulted in neoplastic cells being spread throughout the entire operative site.
The child died the following year.
5th Anniversary Sale!
Subscribe today to get 20% off a standard plan.
CME plan discounted to $395.
You’ll be a better doctor and improve your medicolegal expertise by reviewing cases.
I’ve added a ton of new information to this case.
The most interesting addition is a series of emails that occurred between the surgeon and pathologists in the 24 hours prior to the operation.
Due to the fact that the diagnosis between osteoblastoma and osteosarcoma was unclear, Dr. D (neurosurgeon) sent an email to Dr. V (one of the head pathologists, board certified in anatomic pathology and neuropathology) to discuss the planned biopsy.

Dr. V responded and copied multiple colleagues.

Dr. C responded.

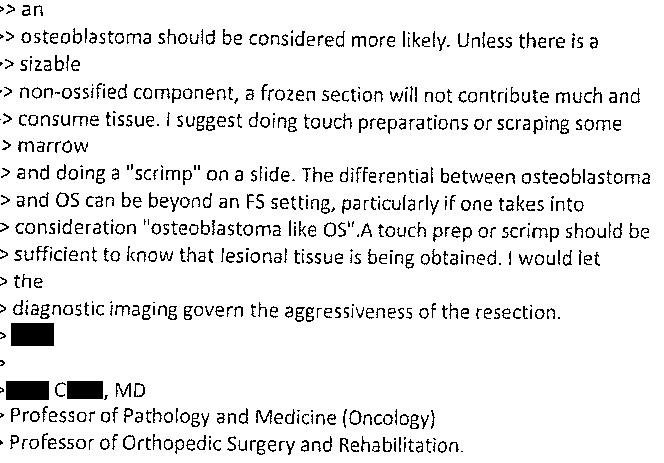
Dr. D replied that the imaging was not giving a clear diagnosis.

Dr. C suggested that instead of having neuroradiologists review it, that the MSK radiology group should give their opinion.

One of the MSK radiologists reviewed the images and emailed Dr. D.
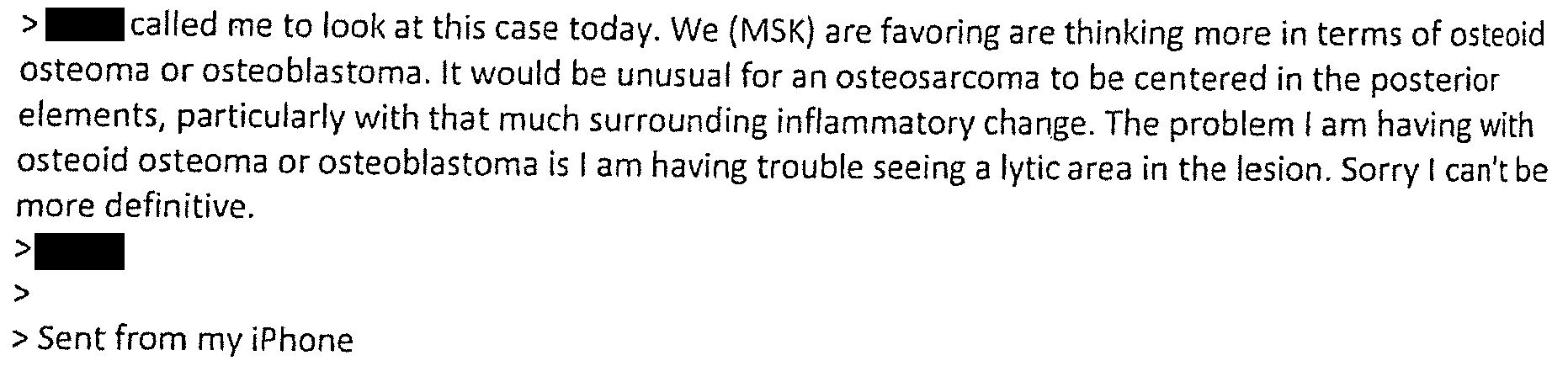
Dr. D responded to the MSK radiologist and copied multiple pathologists involved in the email chain.

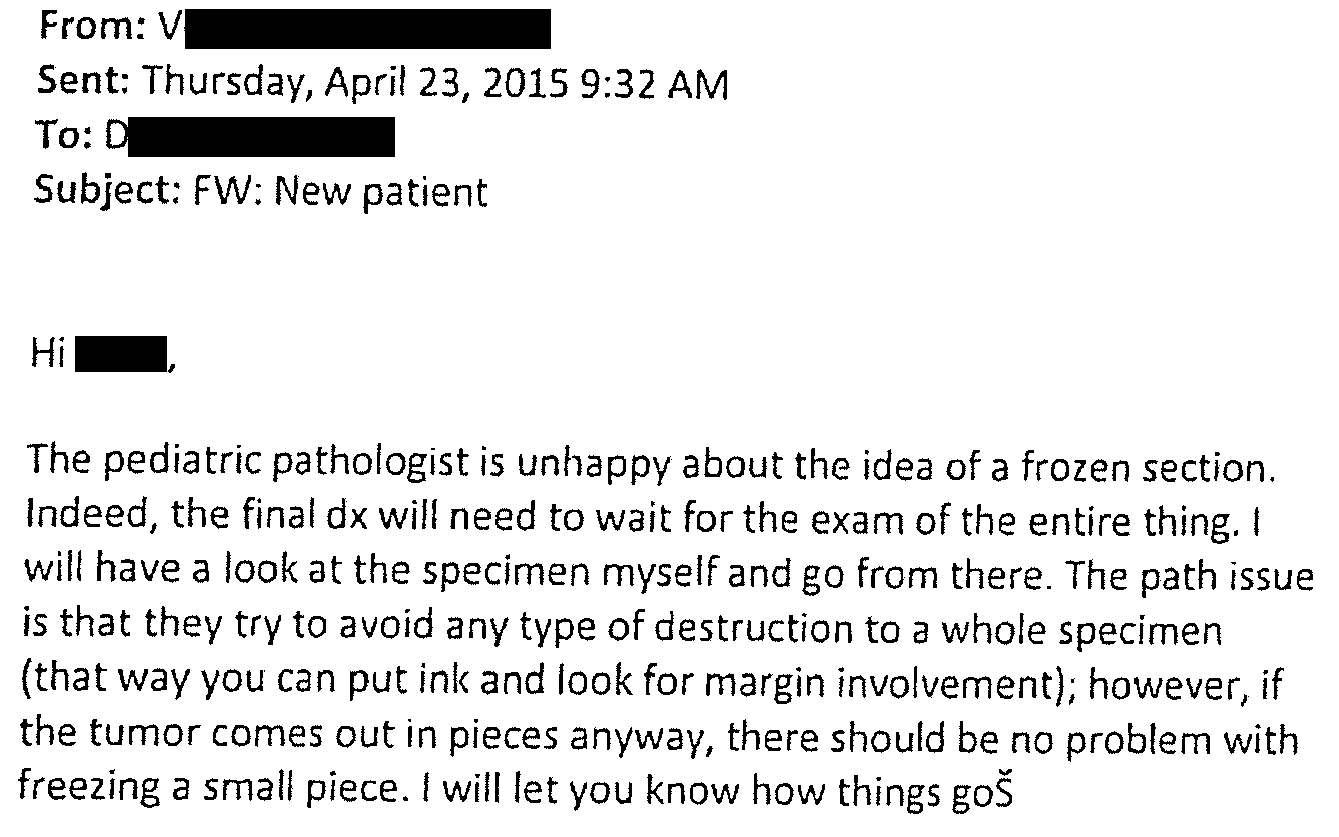
The following day (in the morning before the surgery), a pediatric pathologist wrote this email to the head pathologist (Dr. V) who had been leading communication with Dr. D.

Dr. V notified Dr. D about the pediatric pathologist’s recommendation.
A lot more information was released in the court records about this case.
I’ve added it all to the original post, which you can read here:
assessment/plan from a pediatric heme/onc consult note
full operative report
multiple additional plaintiff and defense expert opinions
final settlement notification
Improve your medicolegal expertise by subscribing.
Now is the cheapest a subscription will be all year.
This is one of the saddest cases I’ve read. A child suffered and died despite the best efforts of a multidisciplinary team. As a father of 3 children it’s hard for me to imagine the anguish of his parents, going from the terror of realizing your child has a mass, to the relief of being told it was actually benign, then to realizing the diagnosis was incorrect and watching him die.
That being said, I’m not sure I can clearly fault the doctors for the decisions they made. The diagnosis wasn’t absolutely definitive, but the odds were definitely in favor of it being osteoblastoma (based on location, imaging results, and initial pathology). Based on the court records, it seems that the final permanent section pathology results were read as being far more likely to be consistent with osteoblastoma than osteosarcoma. Even if the neurosurgeon had waited, the same surgery likely would have been done a few weeks later.
The emails paint a picture of a multidisciplinary team that is being careful and thorough, including multiple different specialists in a coordinated approach.
I don’t think these emails would have necessarily hurt the defendants if the case had gone to trial, but it’s an important reminder that (almost) anything you write about a patient can be discoverable in court, even if written outside the medical record. This is one of those rare risk management points that most of us don’t encounter in our daily practice, but is important to recognize so you’re not surprised when communication you thought was private gets projected on a giant screen in front of a jury some day.
Earlier today I sent a case (to paying subscribers) about an aortic dissection.
The patient had a stable/chronic aortic arch dissection for months… until the day he showed up for the pre-op cath appointment.
He reported a fever, malaise, weakness, shortness of breath, and chest pain to the front desk staff in the waiting area.
After waiting a few hours (his cath was delayed for emergency cases), he coded in the waiting room.
You can read the entire case by clicking on the most recent link in the case archive.