


Dissection After Psych Visit [20% Off Sale]
Case #239

Friendly reminder: The Holiday Sale is going on right now.
Take 20% off an annual subscription.
You’ll be a better doctor and get to see some of the wildest med mal cases that don’t get covered anywhere else.
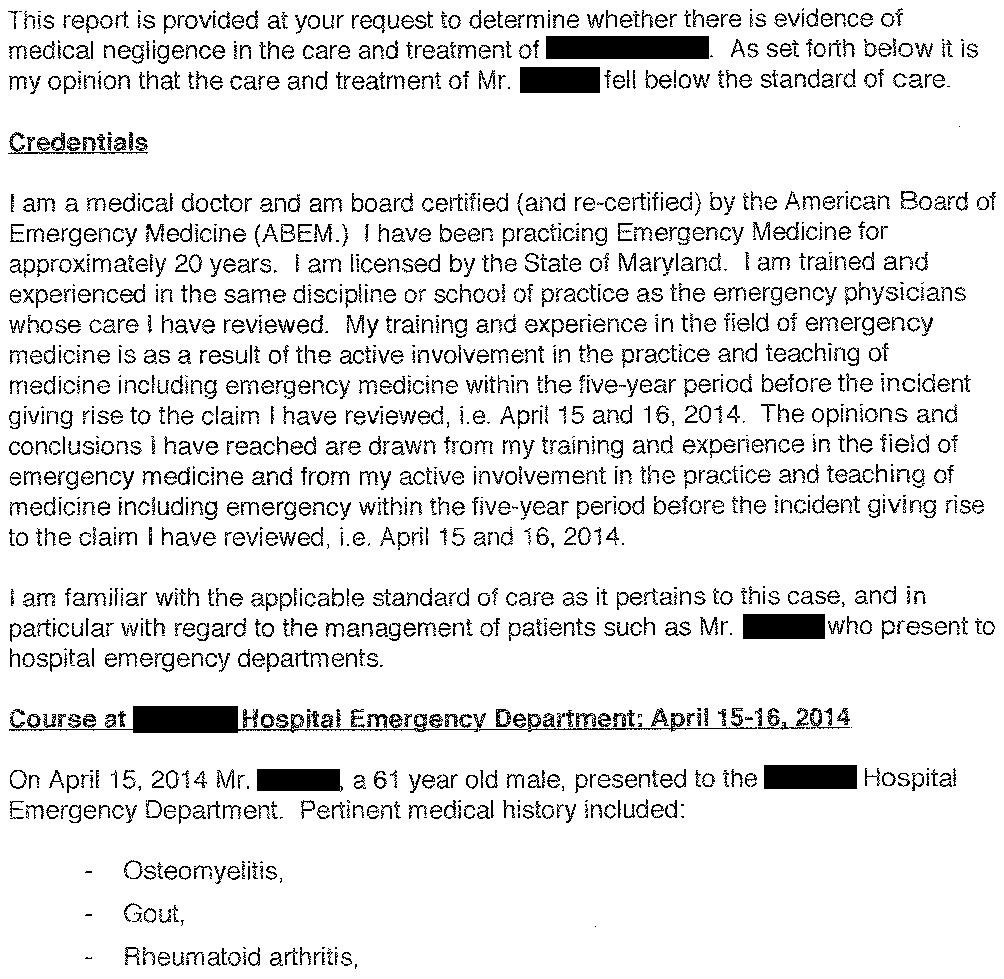
A 61-year-old man presented to the ED, stating that he wanted psychiatric help for his addiction issues.
After discussion with the ED physician (Dr. Wi), it was determined that he was intoxicated, had a long history of alcoholism, and was requesting psychiatric evaluation and placement for alcohol detox.
He had no physical complaints.
Due to his intoxication, he was held overnight in the ED to sober up.
His care was signed out to Dr. K, the overnight ED physician.
Before falling asleep, he requested medication for sleep and pain medication for leg pain.
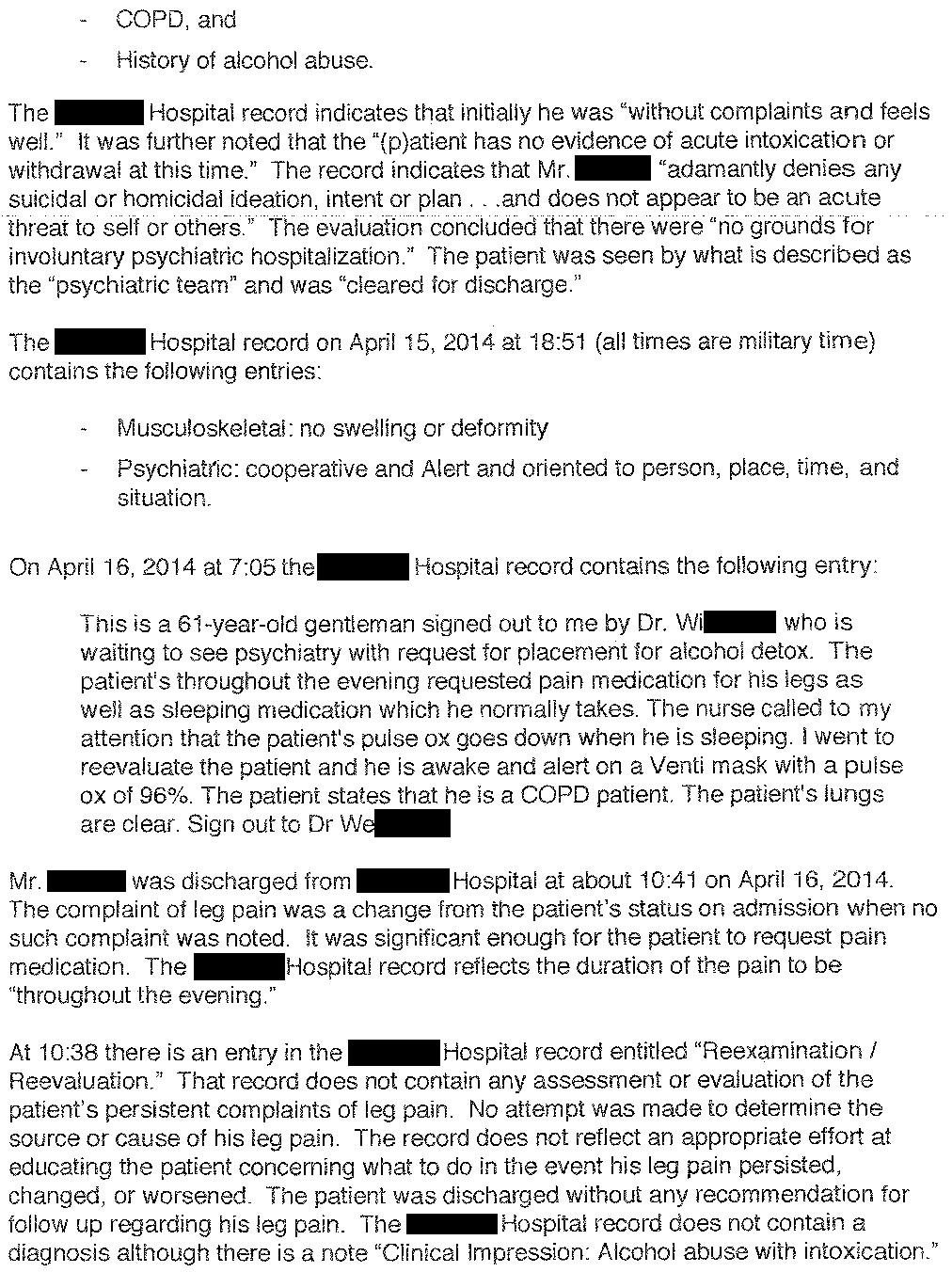
During the night, he was noted to be slightly hypoxic while sleeping and started on supplement oxygen.
His oxygenation returned to normal when he was awake.
The patient had COPD so the physician was not particularly concerned.
In the morning, his care was signed out to Dr. We, awaiting psych evaluation.
He was evaluated by the psychiatric team.
He denied homicidal or suicidal thoughts and was not felt to be a candidate for inpatient psychiatric hospitalization.
He was given information about local alcohol treatment centers, then discharged.
One week later, the patient returned to the ED with right leg pain.
The leg was noted to be necrotic.
CTA showed a focal dissection of the distal aorta extending into the left iliac, as well as extensive arterial thrombosis in the right leg.
Vascular surgery was consulted.
The leg was felt to be unsalvageable.
He underwent a below-knee amputation initially, which later had to be revised to above-knee.
Join thousands of doctors and attorneys on the email list.
The patient contacted a law firm.
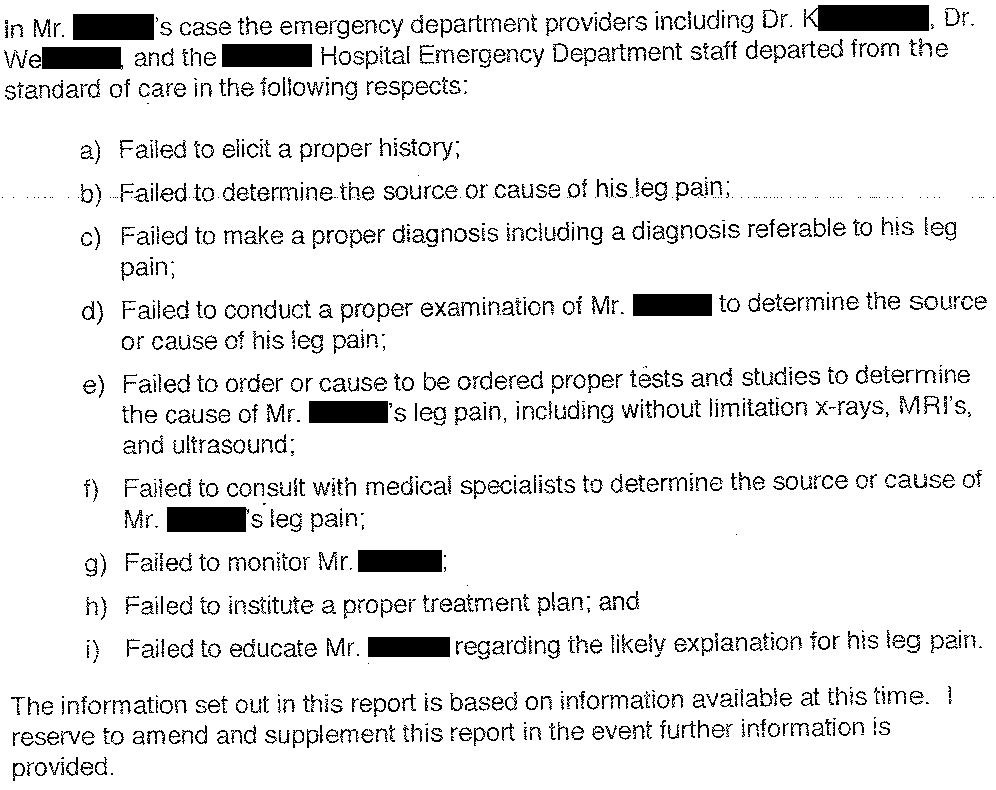
A lawsuit was filed against all 3 EM physicians and their employer.
The primary allegation is that his leg pain during the overnight ED stay was an early symptoms of arterial obstruction, and that it was not appropriately investigated by the ED physicians.
An EM expert witness was hired by the plaintiff:
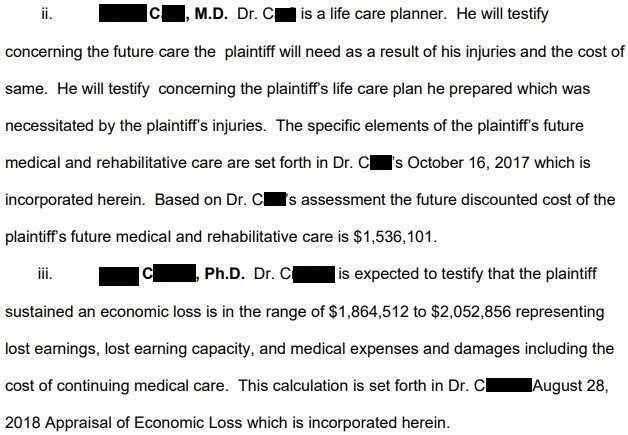
The plaintiff also disclosed experts who estimated ongoing care costs and lost income:
The defense hired an EM expert:
During the lawsuit, the patient was hospitalized with paraspinal abscesses and pneumonia due to Acinetobacter infection
His condition progressed to septic shock and multiorgan failure.
He died before the conclusion of the lawsuit, 4 years after the original ED visit.
The plaintiff hired another expert to claim that his death was a downstream consequence of the missed arterial obstruction and amputation.
The defense hired an infectious disease expert:
I only run 2 sales per year.
This is the best deal you’ll get to improve your practice and get access to the archive of 235+ malpractice lawsuits.
It appears that all of the physicians were removed from the case. Court records did not clarify if they were dropped or if their insurance paid a settlement.
The hospital was the only remaining defendant.
A $5,000,000 settlement offer was made to the hospital.
After negotiations, a confidential settlement was reached and the lawsuit was withdrawn.
MedMalReviewer Analysis:
I’m not convinced the patient even had the dissection or arterial obstruction during the index visit. Even if he did, I think it’s incredibly unlikely that any sane doctor would have made this diagnosis. The pain seems like it was relatively mild (successfully treated with PO pain medication) and he walked out of the ED, which are not hallmarks of acute arterial obstruction. Some patients spout off innumerable new complaints throughout their ED visits, and it’s not possible to re-start a workup from the very beginning each time a patient comes up with a new symptom multiple hours after arriving. The odds of a patient suddenly developing a new emergency totally unrelated to their ED presentation are incredibly low, but it does happen very rarely.
Even if an ultrasound had been ordered, it likely would have been a DVT scan and wouldn’t have necessarily checked the arterial system. If the sonographer happened to note decreased arterial flow, it likely would have been grounds for outpatient follow-up. ER doctors love to order CT scans but even we have our limits; checking a CTA for mild ankle pain in a patient who is in the ED for completely unrelated reasons is beyond ridiculous.
This is a good opportunity to review the ultrasound assessment of arterial obstruction. CTA reports are easy to understand (the read will usually explicitly state if there is an obstruction and if there’s any distal contrast). However, arterial ultrasound reports require some inference which can confuse learners. Arterial ultrasounds usually don’t explicitly identify a clot like a CTA does, especially if the obstruction is very proximal. Even if your patient has an arterial obstruction, the ultrasound report will not state the patient has an obstruction. Most likely, the result will describe a triphasic, biphasic, or monophasic waveform of the distal blood flow. You need to understand what the description of the waveform implies and correlate it with the exam. If you don’t, you will miss the diagnosis like the resident and attending in this case, and the patient will lose their leg.
Checking pulses and capillary refill is important. No one knows if the patient would have had normal foot pulses and capillary refill, but documenting an exam would have helped the doctor’s defense. This requires actually taking the patient’s shoes and socks off, which we often avoid due to the negative olfactory repercussions in unkempt ED patients. For those who are too busy or too lazy to go check themselves, you can ask the nurse to find pulses with a Doppler and make a nurse note (this presumes you actually read the nurses notes and aren’t so rude to them that they avoid coming to tell you they can’t find a pulse).
This may be an unpopular opinion, but the physical exam (excluding simple observation) rarely provides useful information. We often get lazy and skip parts of the exam, and in the vast majority of cases there are no repercussions. However, when the exam does provide useful information, its often the critical piece of information that makes a diagnosis and avoids a malpractice lawsuit. The plaintiff’s attorney will always accuse you of doing a bad exam, no matter what you actually did, so it’s usually an empty criticism. But sometimes it’s a valid criticism.