


Spinal Arachnoiditis After Epidural
Case #17

Ms. L was a 64-year-old woman who underwent surgery to treat rectal adenocarcinoma.
Dr. C was the anesthesiologist during this case.
He placed an epidural catheter as part of the anesthesia administered during the surgery.
Following the surgery, the patient developed paraplegia.
Improve your practice and become a medicolegal expert.
The patient sued the anesthesiologist, alleging that the epidural anesthesia was the cause of her paraplegia.
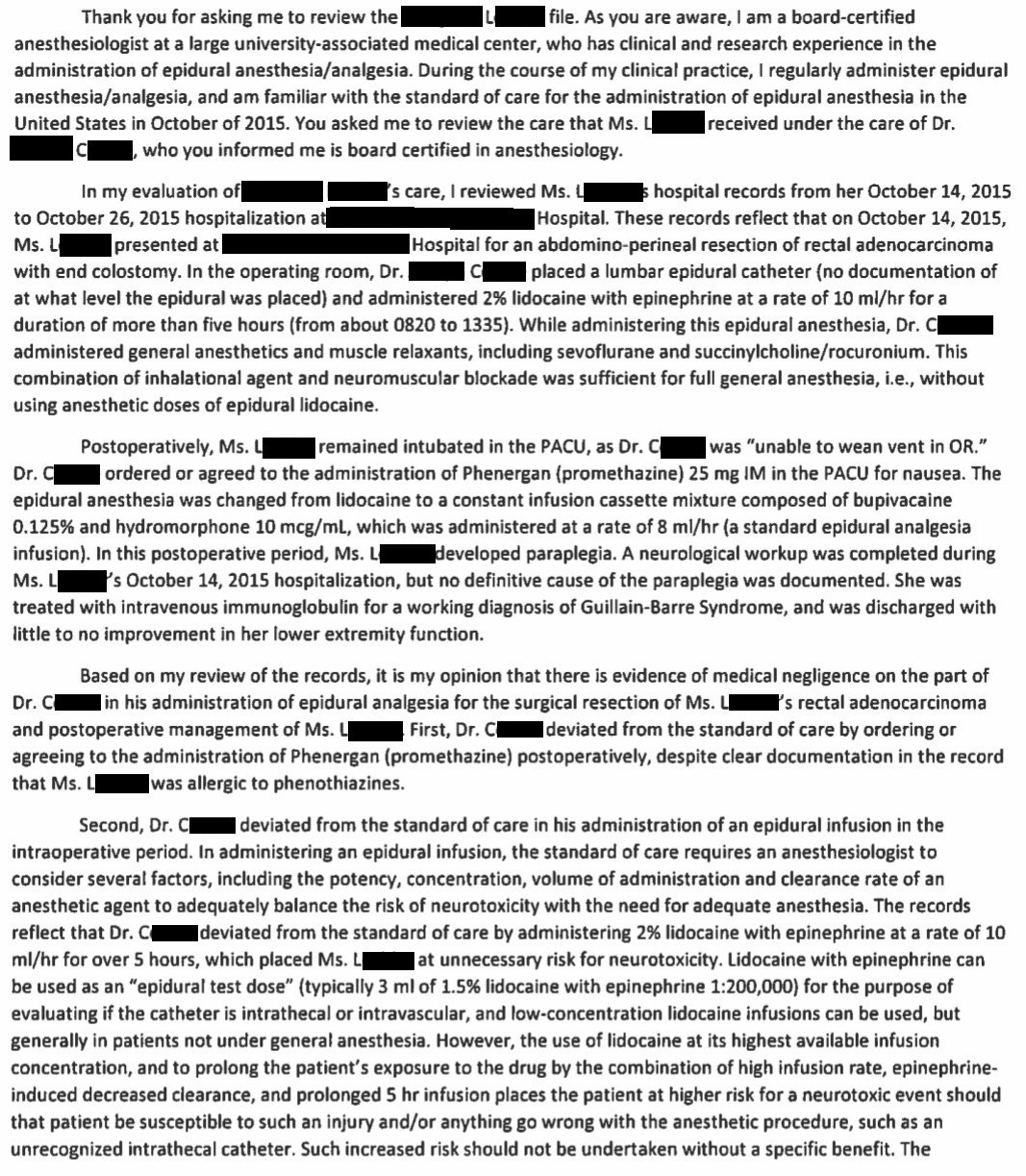
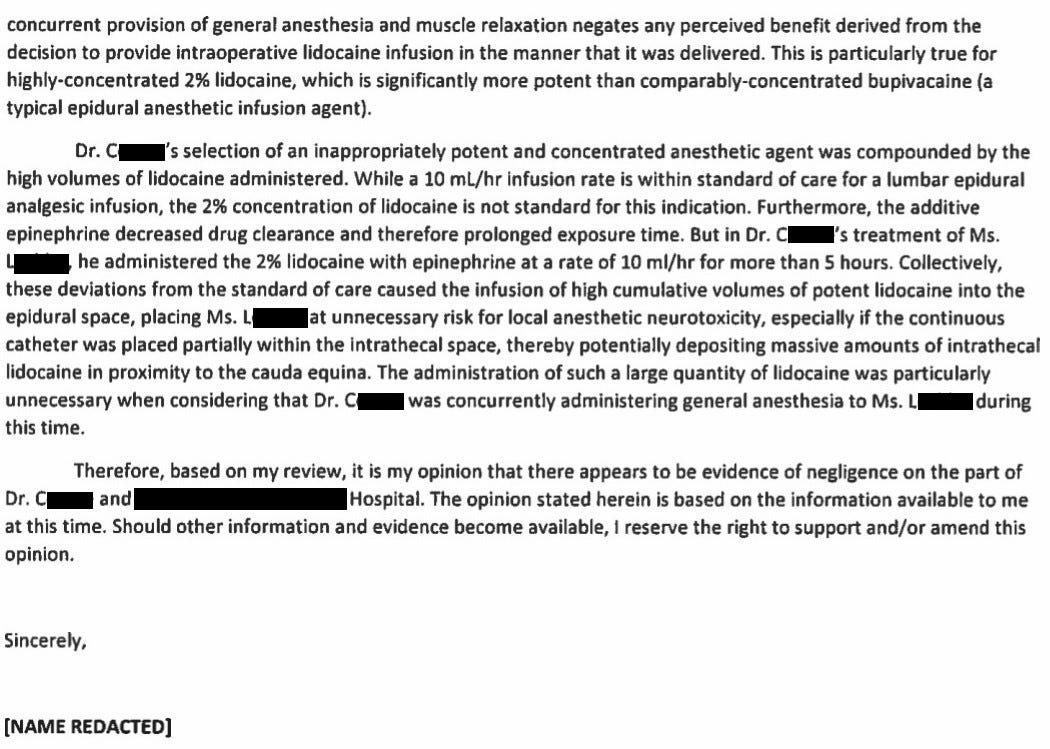
An expert witness was hired and wrote this opinion:
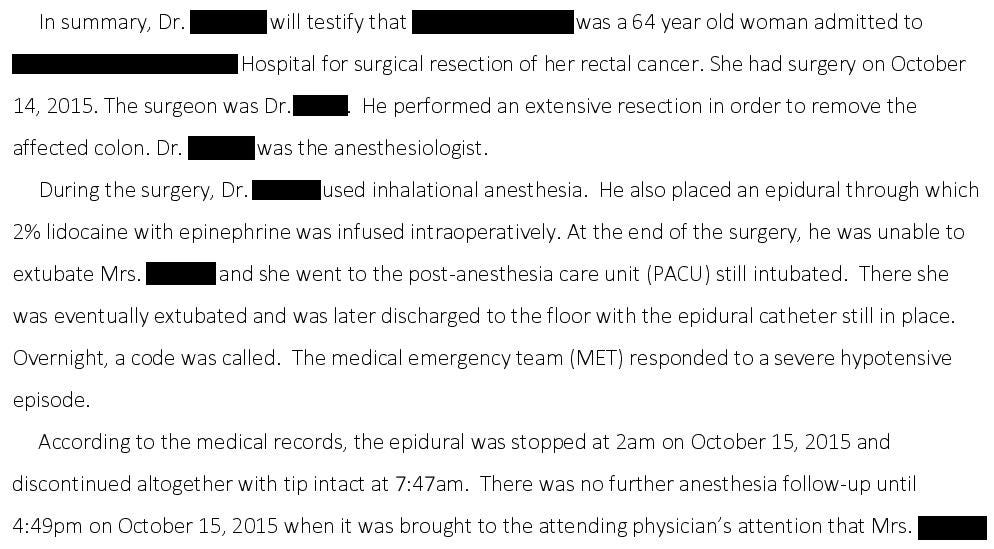
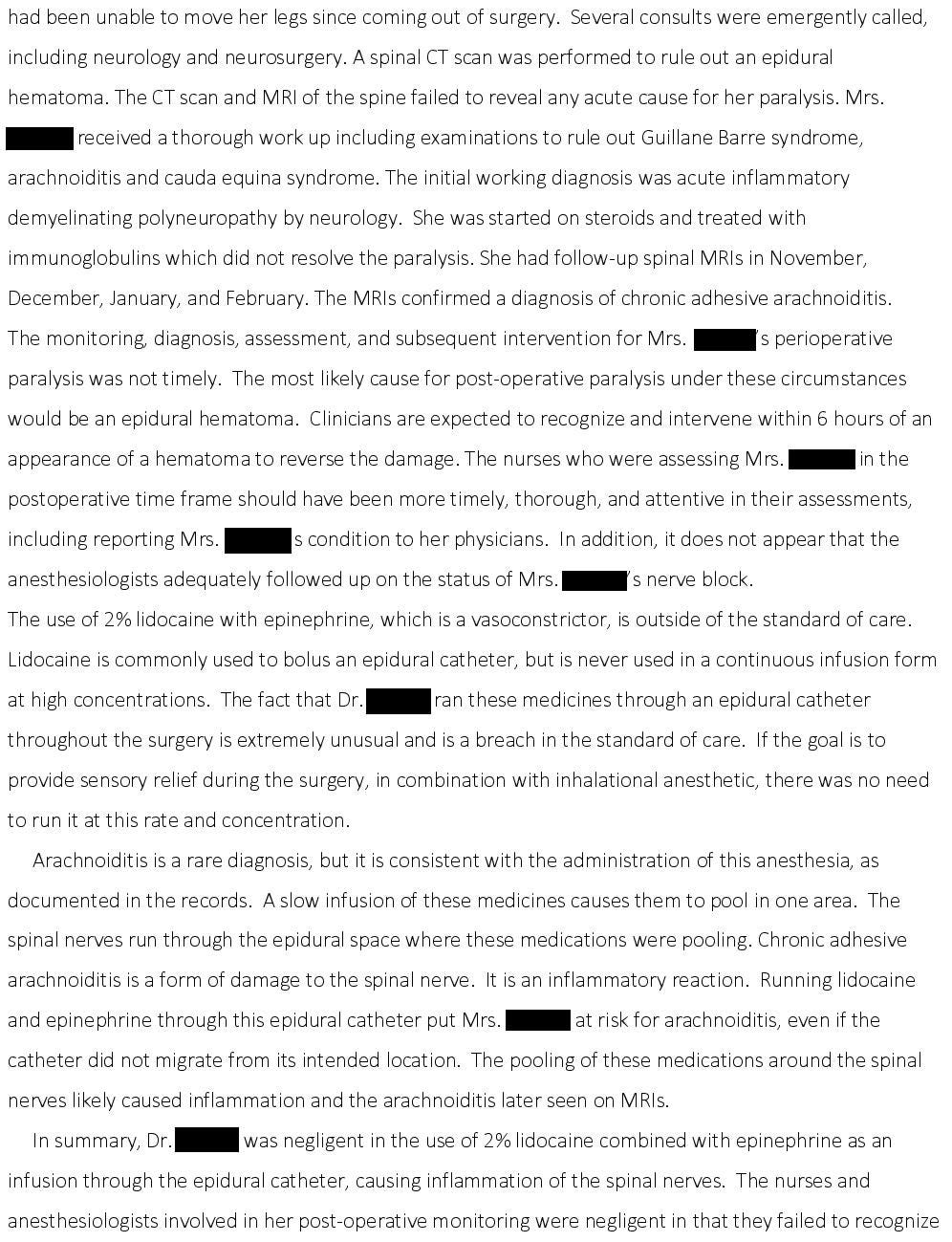
Additional disclosures were made that described the case in more detail:
When I originally published this case, the lawsuit had not been resolved.
It has now been withdrawn after a confidential settlement.
Paying subscribers get a new case every week and access to the entire archive.
MedMalReviewer Analysis:
The working diagnosis of Guillan-Barre Syndrome is somewhat suspect. The odds of a patient undergoing a large surgery with epidural anesthesia and incidentally developing Guillan-Barre Syndrome at the same time is incredibly low.
To be frank, I had never heard of arachnoiditis previous to this case. This is a nice case report and overview related to a case that occurred after an obstetrical epidural. One of the reasons I love reading medical malpractice cases is that it exposes me to rare diagnoses outside my field and broadens my knowledge.
There is a valid criticism that the patient should not have been given Phenergan if there was a documented allergy, but it almost certainly had nothing to do with the patient’s paralysis.
This was my original analysis in 2020 when I published this case: “I expect this case to be settled prior to trial. The patient has a permanent disability that was almost certainly iatrogenic. The plaintiff will likely find a sympathetic jury, and the defense would be wise to settle rather than risk a massive financial liability".” Its taken several years but my original analysis has proven correct.
If you’re interested in reading more cases, check out Case #16 (for subscribers only).
A cardiothoracic surgeon was removing a mediastinal mass when the left subclavian artery was injured.
It was ligated and the surgeon initially believed there was good collateral flow.
However, 24 hours later the patient was diagnosed with an ischemic limb, and a vascular surgeon performed a carotid-subclavian bypass.
The following day the patient was diagnosed with compartment syndrome and a hand surgeon did a bedside fasciotomy.
The patient’s arm was saved but he suffered a permanent disability.

The lido infusion is unorthodox, but I would say doses still clinical. Wonder what the imaging shows. If
Acute arachnoiditis can also be caused by high-concentration chlorhexidine injection into the epidural space. https://pubmed.ncbi.nlm.nih.gov/30447665/