

Lumpectomy Misses Cancer
Case #241

A 51-year-old woman underwent a regularly scheduled mammogram.
The results showed a 6mm spiculated lesion in her right breast.
She was referred to an interventional radiologist for biopsy.
The IR physician performed an ultrasound-guided needle biopsy, and placed a clip for subsequent localization.
The biopsy confirmed invasive ductal carcinoma, grade 2, ER +, PR +, Her2neu -.
The patient was referred to a surgical oncologist.
She was seen by Dr. L.
After discussion of options, the patient elected for a lumpectomy.
Join thousands of doctors and attorneys on the email list.
Free and paid options available.
The surgery was completed without any initial complications.
The surgeon documented the following:
It was later determined that the cancer (and clip) had been missed and was still located in her breast.
The patient went to a different surgeon, and the lumpectomy was completed.
Due to the large volume of missing breast tissue, she also underwent bilateral reduction mastiopexy to achieve symmetry.
The patient filed a lawsuit against the surgeon and the hospital.
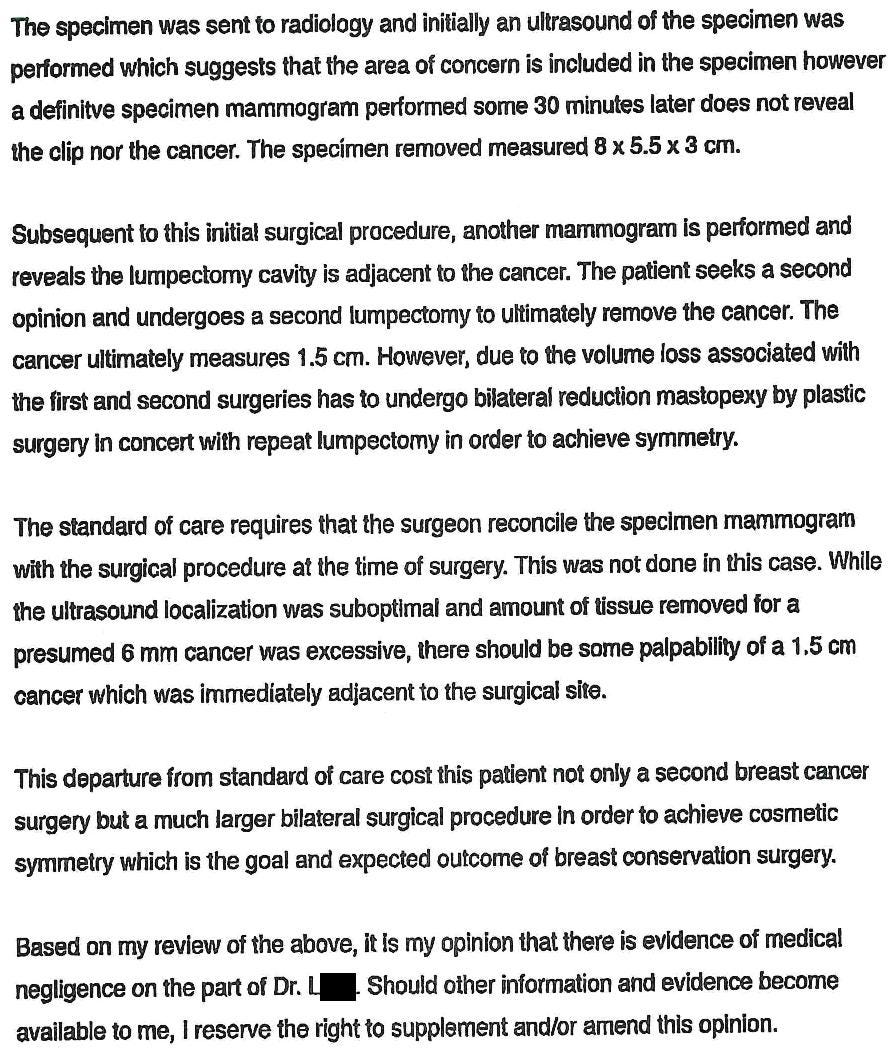
The expert witness opinion is shown here:
Become a better doctor and expand your medicolegal expertise.
Paying subscribers get a new case every week and access to the entire archive.
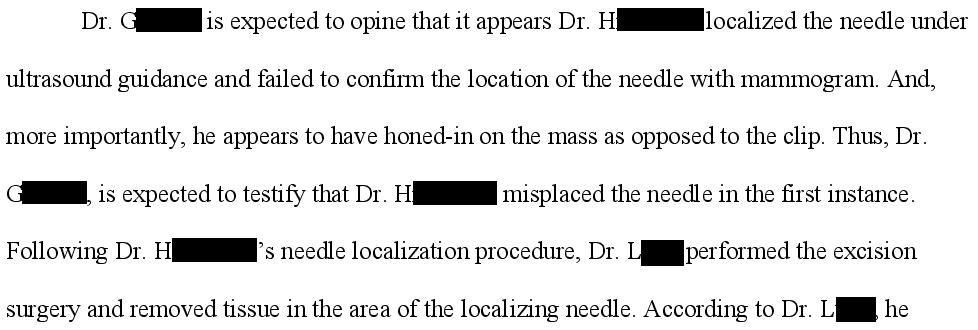
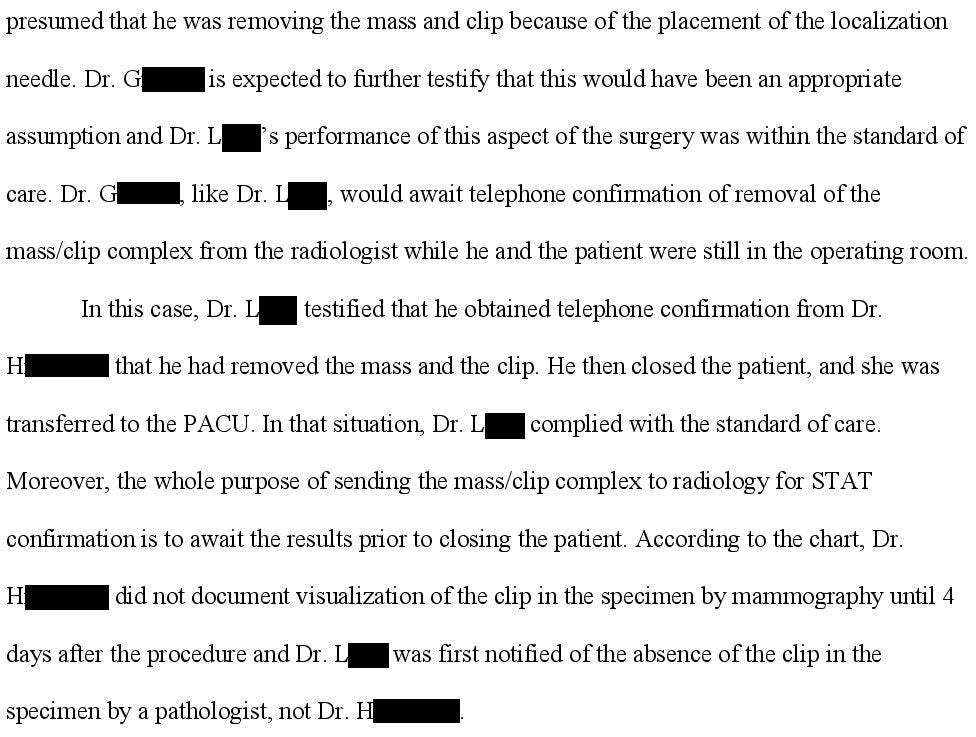
The defense hired their own surgeon expert witness Dr. G).
He provided critical information that the plaintiff attorney left out.
Apparently, a radiologist (Dr. H), had done the peri-operative mass localization and was supposed to have done post-surgical imaging of the specimen, which was not done.
The lawsuit is ongoing.
I will update subscribers as new developments happen.
MedMalReviewer Analysis:
The defense expert’s description of the radiologist’s actions completely reverses the analysis of this case. I find it incredibly dishonest that the plaintiff’s attorney and expert decided to leave out this critical piece of information, in an attempt to blame the surgeon. The most charitable interpretation would be that there was a verbal miscommunication between the radiologist and surgeon. The other possibility (that the radiologist told a bald-faced lie) is extremely bad.
Surprisingly, the radiologist was not named in this lawsuit. Sometimes attorneys will file a separate lawsuit for each defendant, so I did a thorough search for any other lawsuits related to this one, but none were discovered. The only other option that could possibly explain the lack of a lawsuit against the radiologist was that they reached a settlement prior to filing a lawsuit. I wish we could get the radiologist’s side of this story, but unfortunately I doubt we will ever know.
I think one valid take-home point from this case (regardless of what happened between the surgeon and radiologist) is to review the images that you order. Sometimes a verbal or written report from a radiologist may be lacking critical information. I don’t intend to demean radiologists, but all doctors make mistakes form time to time, and we provide better care when we collaborate and have 2 sets of eyes reviewing images.
In some ways this case was a miss, but in some ways, the system worked and the error was reversed relatively quickly. Everyone involved owes the pathologist who realized the mistake a very nice Christmas gift. I understand the patient’s frustration about having to undergo a repeat operation and having a poor cosmetic outcome, but it could have been a lot worse if the mistake had gone unrecognized and her cancer metastasized. I covered a previous case in which something similar happened, when a uterine biopsy allegedly failed to obtain adequate tissue and her cancer was missed.
I’ve covered a few other breast-related cases:
I will accept said christmas gift on behalf of my colleagues
Now for a serious comment: Where I trained (thankfully I don't do these anymore) indeed it was standard practice even for us to review the intraop imaging ourselves to make sure we could see whatever seeds/clips/wires were reported to be in the specimen prior to touching it. We even had our own little x-ray machine to take our own images of the specimen before grossing to again confirm everything is there because it has happened that things fall out between radiology and the gross room.
Depending on the setup, if the pathologist didn't have access to the EMR, this must have been an absolute nightmare of a case because they've been told the specimen has a clip and cancer in it and then they can't find it. At what point were they finally confident enough that it simply wasn't there? What a phone call that must have been to the surgeon and/or radiologist.
You nailed it that while the patient did suffer some harm, the harm that was *avoided* was potentially devastating and fatal.