
Professional Athlete Splenectomy
Case #229

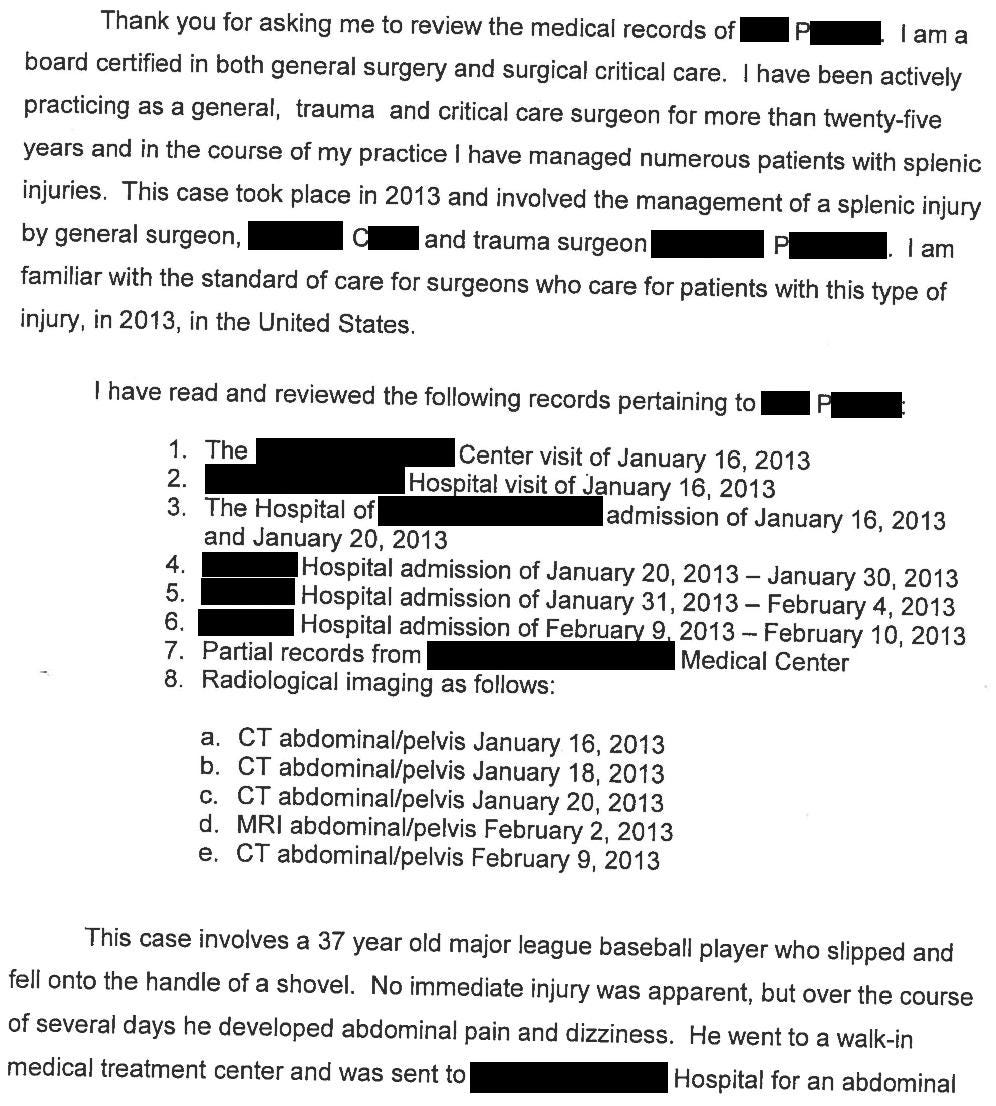
A 37-year-old man was shoveling snow off his driveway when the handle of the shovel struck him in the abdomen.
He was a major league baseball player.
Over the next few days he developed abdominal pain and dizziness.
At a nearby hospital, he underwent a CT scan that showed a grade IV splenic laceration and hemoperitoneum.
The patient was transferred to another hospital with better surgical capabilities.
As he was stable, conservative management was recommended.
However, his hematocrit trended down from 39 to 21.
A repeat CT scan showed worsening hemoperitoneum.
The surgeon felt he may be a candidate for splenic artery embolization, so the patient was transferred to a third hospital that had IR.
Join thousands of doctors and attorneys on the email list.
The interventional radiologist reviewed the case and recommended an embolization.
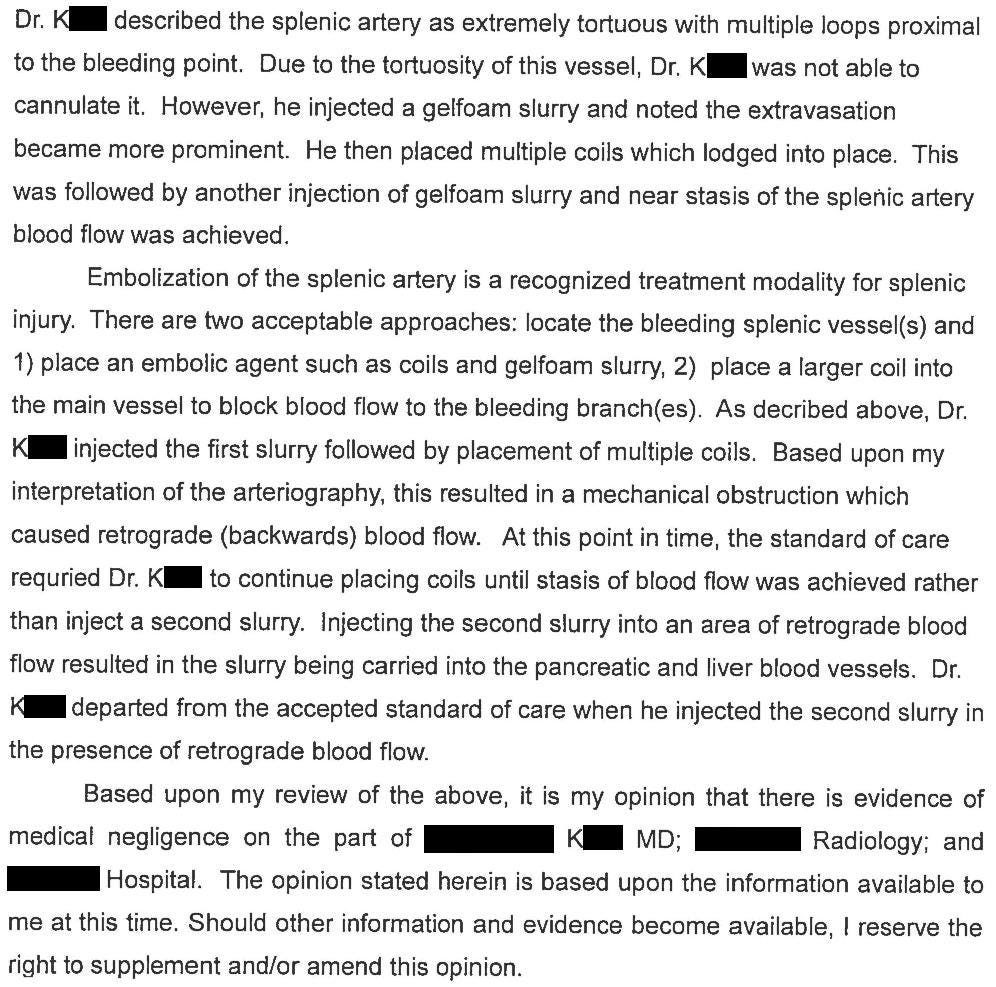
It was a challenging procedure complicated by tortuous vessels.

Following the embolization, the patient’s pain worsened and he developed distension.
The trauma/critical care surgeon (Dr. P) asked a hepatobiliary surgeon (Dr. C) to consider if he could do a minimally-invasive approach.
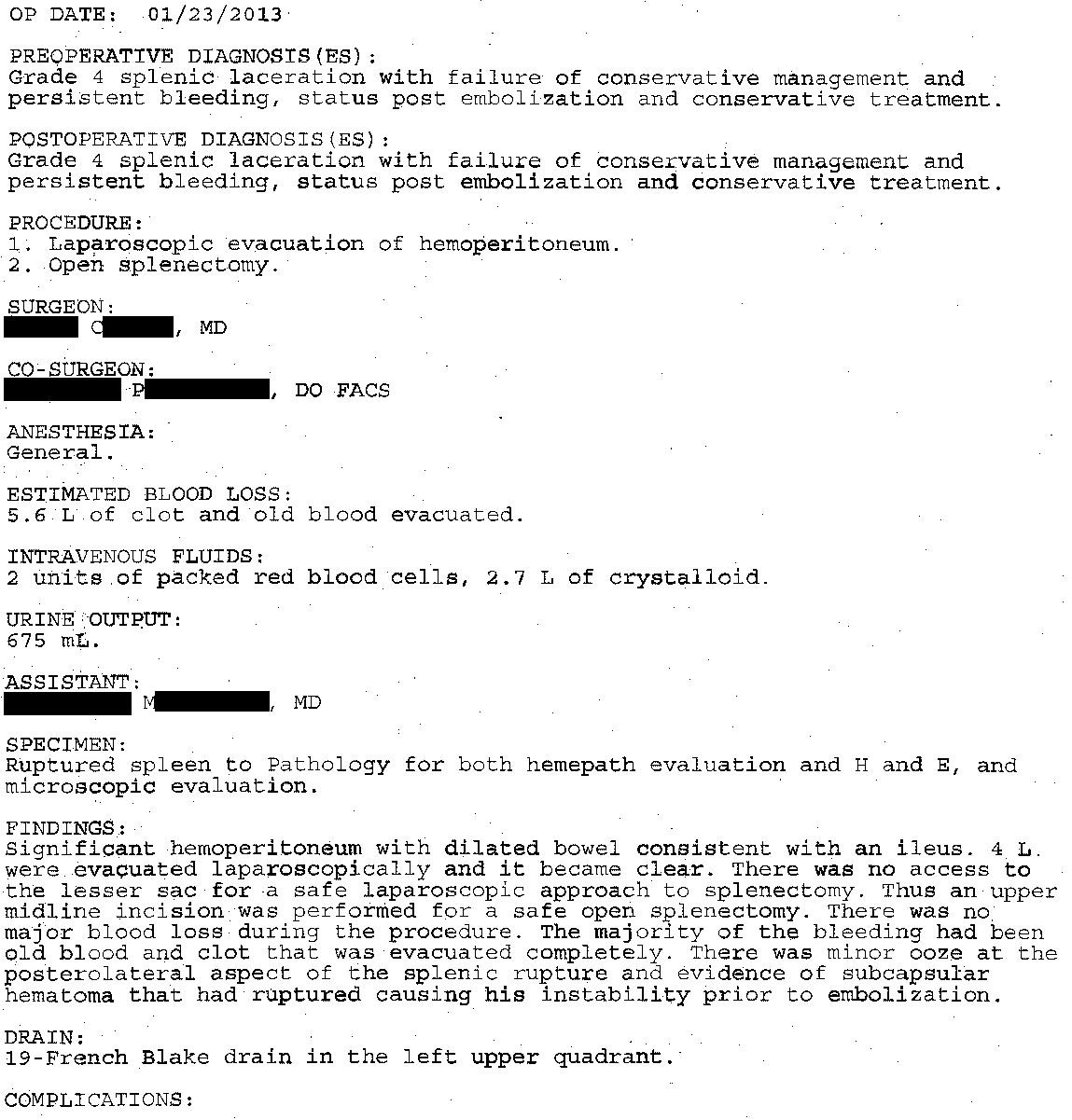
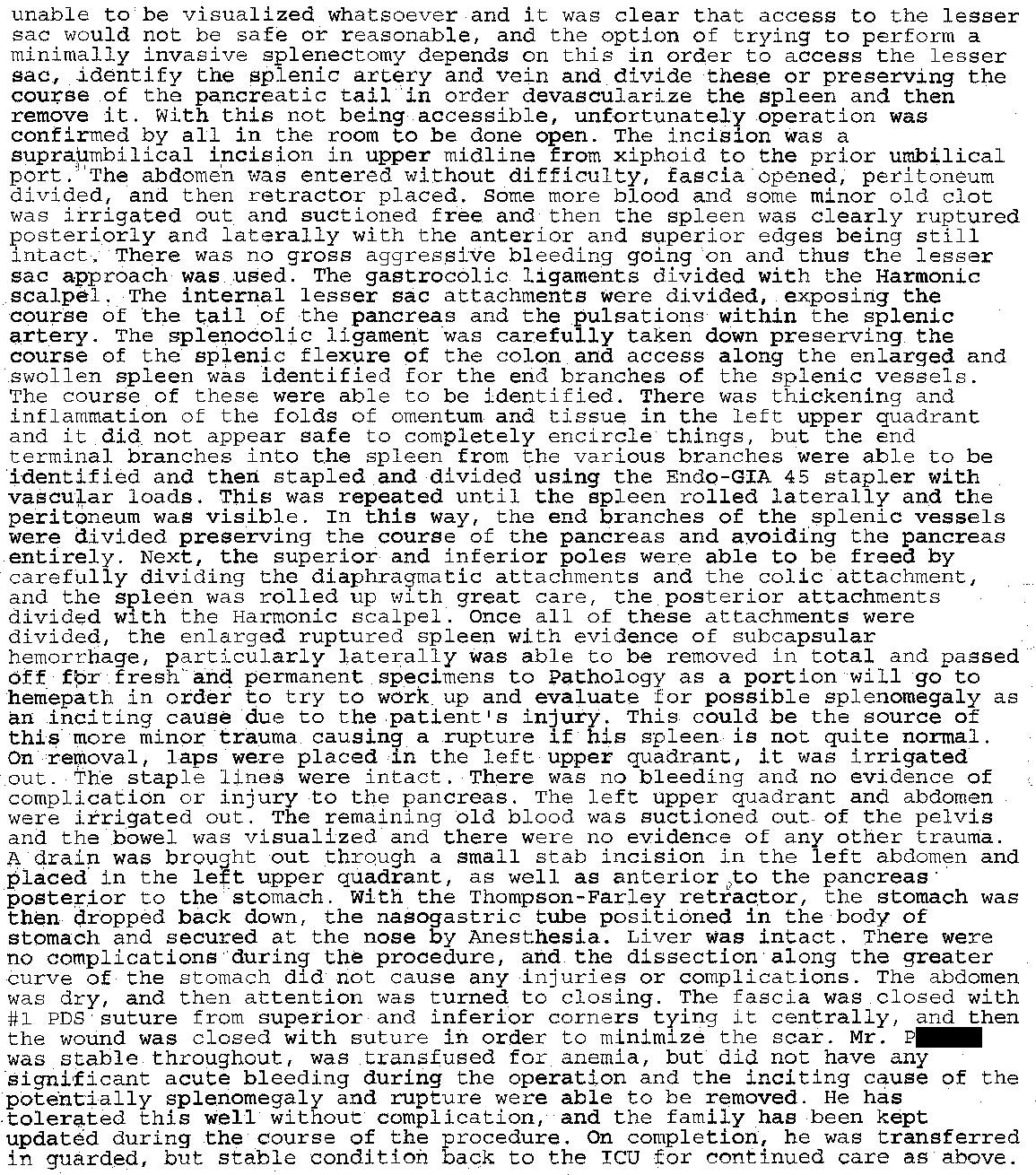
2 days after the embolization, they took him to the OR for a splenectomy.
The patient had numerous post-operative complications including a large pleural effusion that required thoracentesis.
Repeat CT scans demonstrated necrotic pancreatitis, a peri-pancreatic fluid collection that was drained percutaneously, and ultimately he underwent a distal pancreatectomy.
The working theory was that the gelfoam slurry used in the IR procedure had accidentally embolized into the vasculature of the pancreas and liver.
The patient survived but he was never able to play professional baseball again.
He and his family filed a lawsuit against the interventional radiologist and his radiology group, the hepatobiliary surgeon, and the hospital.
The plaintiff’s interventional radiologist expert wrote the following opinion:
Become a better doctor by reviewing malpractice cases.
The plaintiff’s general surgery expert wrote the following opinion:
Note that only Dr. C (hepatobiliary surgeon) was named as a defendant in the lawsuit, not Dr. P (trauma/critical care surgeon).
The plaintiffs reached a settlement with Dr. C and the hospital.
The lawsuit continued against the interventional radiologist and his group.
The defense hired their own IR expert, who claimed that the pancreatic injuries and complications were a result of the splenectomy, not the embolization.

The defense hired an orthopedic surgeon sports medicine specialist to indicate that the patient’s baseball career was essentially over prior to his spleen injury.
This specialist works for a major league baseball team.

They also hired a sports economist to elaborate on his expected contract.
The patient’s lifetime earnings from his professional contracts were also disclosed:

Paying subscribers get a new case every week and access to the entire archive.
Subscribe today and become a medicolegal expert.
Finally, a meteorology expert was hired.


Shortly before trial, the two sides reached a confidential settlement.
MedMalReviewer Analysis:
I find it quite bizarre that the hepatobiliary surgeon was sued. He did not cause the complications and seems to have provided excellent care to the patient. The plaintiff’s expert claims that the injury to the pancreas should have been visible during the splenectomy, but the surgeon literally checked for this and did not find any sign of it. Its hard to understand how an expert can be so arrogant and out-of-touch to believe that he knows better than the surgeon who actually inspected the patient’s pancreas. The expert also suggests that the pancreas should have been debrided or resected (despite appearing normal), violating one of they key maxims of surgery: “don’t mess with the pancreas”. Its one thing for an expert to offer biased and untrue testimony in a medical malpractice case, but its the peak of irony to suggest a course of action that itself would likely be malpractice.
It seems a bit unusual that a professional athlete would suffer a spleen rupture from a shovel handle. The mechanism seems fairly minor and the patient was young and fit. I wonder if he had mono (or other underlying spleen pathology) or if it was just a freak accident. Unfortunately they did not include the path report or any other labs in the court records.
I’m not an interventional radiologist so its not clear to me if doing a second injection of gelfoam slurry is substandard or known to be particularly risky. I can certainly understand how a desire to help the patient avoid a splenectomy and not have the embarrassment of a failed procedure could lead to some pressure to be aggressive.
This is the first case I’ve seen that involved a meteorologist as an expert witness. I can’t figure out what the defense was trying to do by disclosing this expert. They’re suggesting that the patient did not actually need to be shoveling snow that day, but the mechanism of injury doesn’t seem relevant to me. Even if the patient lied about how he suffered the injury, I can’t imagine how this would help the defense besides character assassination of the defendant.
This case has a few parallels to a recent case that got a lot of attention in the media in which a surgeon attempting to do a splenectomy accidentally removed a patient’s liver. Both had subacute presentations that did not mandate immediate operative intervention, but had slowly declining hematocrits that eventually prompted a splenectomy. Both surgeries started laparoscopically then were converted to open. The risks of both IR embolization and operative interventions are on full display in these cases.
This lawsuit reminded me of a previous (subscriber) case I covered in which a patient presented with severe headaches and had a CTA head in the ED.
An interventional neurologist attempted to coil a 7x4mm ACA aneurysm.
The first coil was placed without issue, but the second coil accidentally knocked the first coil out of place, into the ACA itself.
The interventional neurologist called an interventional radiologist for help, but after multiple attempts they were unable to get the coil out.
The patient suffered a significant stroke, had a craniotomy, and was left with permanent disability.
You can read it here:
I can imagine a shovel handle doing this. The incident is not precisely described anywhere, but people don't like to fall & will perform amazingly athletic moves trying to not fall. And this was a young athletic man & may have been on slippery or uncertain footing. If the shovel had been stuck in the snow or laden with snow, I can picture his body falling forward or sideways & undergoing contortions. It would be not at all impossible for the end of the handle to be jutting upwards & jab him strongly in the LUQ. I've seen something quite similar:
I made rounds at 7 AM one day as an intern & an elderly female patient on my general surgery service looked well & had no new complaints. At that hour in Canada it is dark. At 4 PM the same day I rounded with the staff surgeon, in daylight, & we were shocked to see she was as white as a ghost. Only then did she report she'd gotten up to pee in the night & fallen, striking her LUQ against the corner of the footstool by her bed. Her Hb was 6 by 4 PM. The surgeon did a splenectomy. So weird things happen !
Interventional techniques are invaluable but I often wonder if IR do not at times persist for too long using increasingly aggressive techniques to fix what their initial attempts failed to fix. Not only that, something similar seems to be happening in the O.R., where surgeons seem so married to the idea of doing something using minimal access techniques, that they are choosing too late to convert to an open procedure. Is anyone else thinking this?
Honestly the question of whether the IR doc was negligent depends on how common it is to accidentally compromise pancreatic blood supply during a splenic embolization. This is a very technical question which as an EM doc i have no idea what the answer is - and of course the jury has even less of an idea. If the procedure was that difficult as described in the report it may have been better to abort and just do the splenectomy but again this seems like something you need to be highly specialized to be able to adjudicate.