


Recurrent Laryngeal Nerve Injury [Thyroidectomy]
Case #247

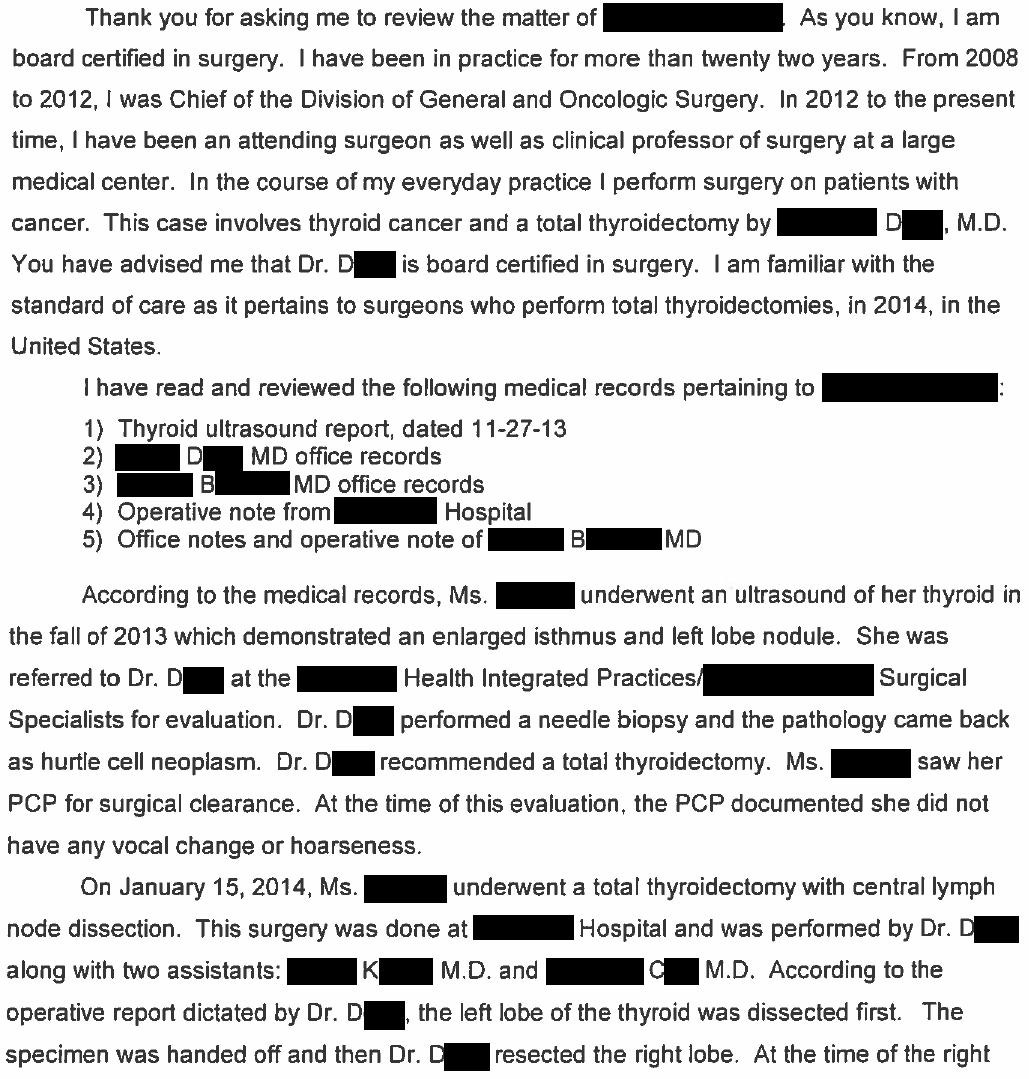
A woman noticed a lump on the left side of her anterior neck.
Thyroid ultrasound revealed a nodule.
She was referred to Dr. D, a general surgeon.
A needle biopsy was done and showed a Hurthle cell (oncocytic) carcinoma.
Dr. D discussed the results and recommended a total thyroidectomy.
During his discussion with the patient, he discussed the risk of recurrent laryngeal nerve injury, and the written consent also mentioned this.
The patient took Dr. D’s advice, signed the consent form, and scheduled the surgery.
The surgery itself was uneventful.
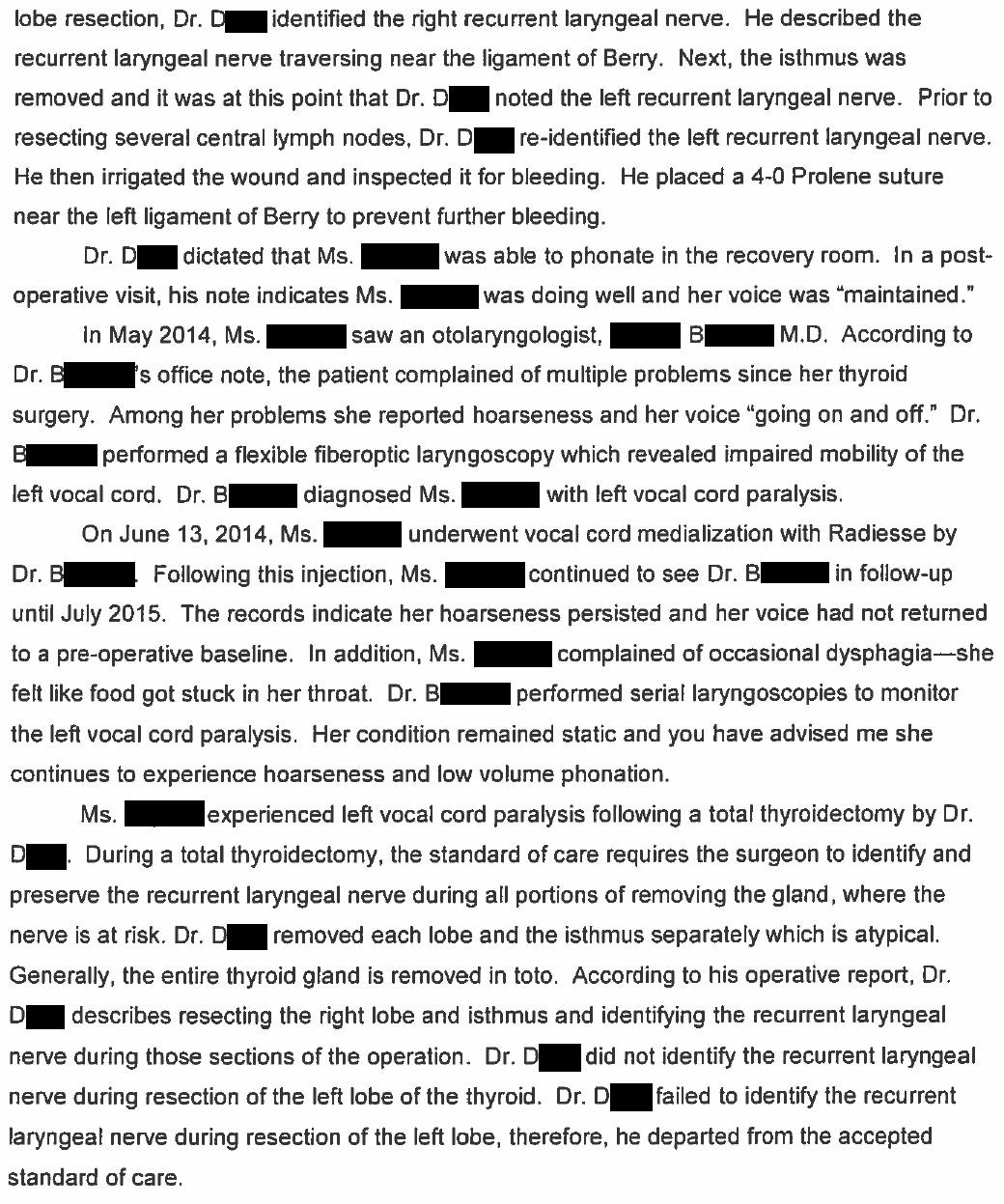
In the PACU she was able to speak without noted difficulty.
At home the patient developed difficulty speaking.
She saw an ENT physician (Dr. B) several months later.
Laryngoscopy confirmed left vocal cord paralysis.
A medialization procedure was done by Dr. B but she continues to have issues with vocalization.
Become a better doctor by reviewing malpractice cases.
It’s free to join the email list, and paid options are available for those who want to expand their medicolegal expertise.
The patient and her husband contacted a law firm.
They sued the hospital itself, but did not sue the general surgeon nor his employer.
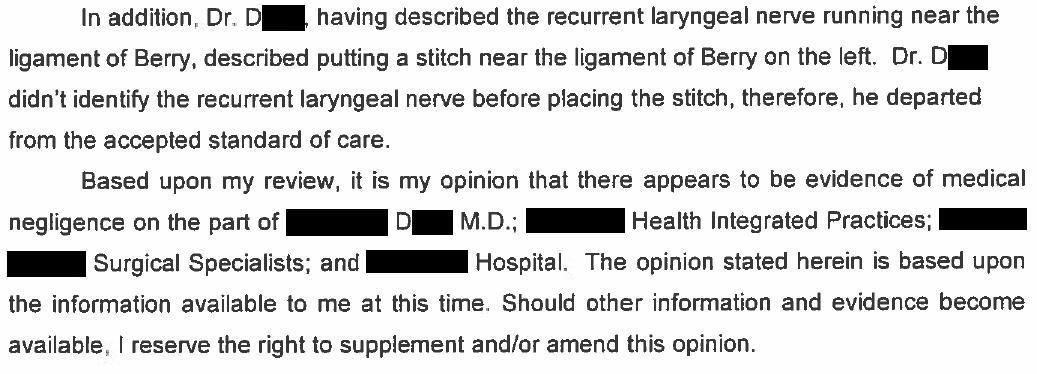
The expert opinion is shown here:
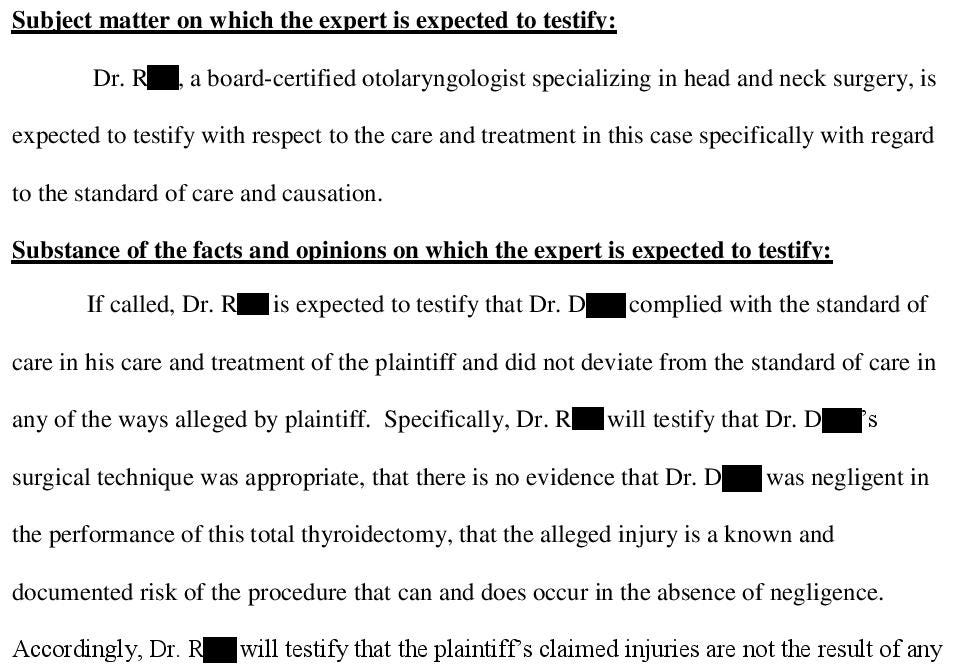
The defense hired their own expert.

The plaintiffs offered to settle with the hospital.

The hospital refused the settlement offer.
The plaintiff filed a motion asking the judge to ban any mention that this injury was a known risk of the procedure.

The defense filed a response in opposition to the plaintiff’s motion in limine.


The referenced deposition excerpt is shown here, this is the only part of the deposition that was included in the court records.

Learn from malpractice cases to reduce the likelihood of getting sued yourself.
Paying subscribers get a new case every week and access to the archive.
The judge did not make a pre-trial ruling about the motion in limine seeking to prevent discussion of the “risk of the procedure”.
After deliberating, the jury returned a verdict for the defense.

MedMalReviewer Analysis:
I’m surprised that the law firm took this case. The defense had the upper hand from the beginning and I would have been very surprised if the jury had ruled for the plaintiff. I’ve seen a good number of other lawsuits from this firm and they usually only take cases where there is fairly clear malpractice. They ended up losing a good deal of money bringing this lawsuit which will hopefully discourage them from this behavior in the future.
Even though the defense won, this case is a good reminder that an informed consent is not a get out of jail free card. Just because you consent a patient for a particular complication, doesn’t mean they can’t sue when that complication occurs. Informed consent presumes you are operating within the standard of care. If you discuss the possibility of a recurrent laryngeal nerve injury and then perform the surgery negligently and cut straight through the nerve, you can still be found liable.
The patient’s primary language is Spanish, and an interpreter was requested for her and her husband at trial. This made me wonder if they were going to claim that the doctor should have used an interpreter for consent, but they did not raise this issue at trial.
The surgeon’s documentation played a key role in his defense. He documented their discussion in his note and also had a signed informed consent. It didn’t prevent a lawsuit but it really helped the defense attorney argue their case and was an absolutely critical key to their victory.
I’ve covered a previous lawsuit involving a general surgeon doing a neck procedure that caused a nerve injury. It included an operation on a lateral neck mass that injured the spinal accessory nerve. Even if you don’t do these procedures, patients with these complications may not know where to turn and can end up in your clinic or ED. It’s always worth reviewing these issues that are technically outside of your specialty so that you can become a better clinician.
I probably answered some questions about Hurthle cell (oncocytic) carcinoma on a test during medical school but I had completely forgotten about it. If you’re like me and could use a good refresher, I thought this article was well done.
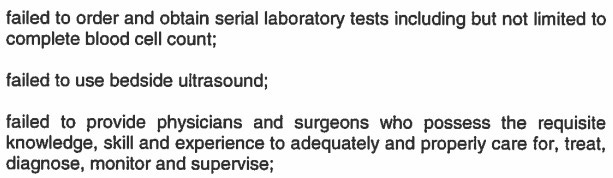
Last week’s case for paying subscribers was about a catastrophic abdominal and retroperitoneal hemorrhage.
The ED physician (pulm/crit doctor covering the ED) was accused of not doing a FAST scan, not giving any blood even after realizing the patient was in hemorrhagic shock, and starting dopamine.
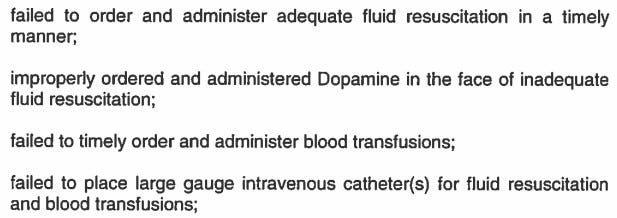
It went to a jury trial with a bizarre ending that was appealed.
If you missed it, you can read the entire case here:

Unless any surgeons want to chime in on something I'm not getting, seems like a pretty horrendous case to bring. Just about any medical student could tell you that this is *the* well-established complication of a thyroidectomy even done correctly. Absent a blithe disregard for the nerve (which doesn't sound supported by the documentation) this should be a very difficult case to win before any sane jury. I'm glad the hospital didn't cave to the settlement pressure and sent the law firm packing with a sock in their mouth.
The motion to prevent discussion of this being a known result of non-negligent thyroidectomy is pretty wild and imo gives away the game that this was an attempt to monetize a bad outcome.
This reminds me of your case where an oncologist literally cured someone's cancer but got sued over a temporary side effect of bleomycin (from which the patient recovered).
The plaintiff expert's report seems self-contradictory. It points out that Dr. D describes or notes each recurrent laryngeal nerve, but then says Dr. D failed to identify the left recurrent. The plaintiff firm misjudged, and the plaintiffs themselves might have been ambivalent anyway having sued just the hospital and not the doctor.