


Suicide After Wife Requests Divorce
Case #189

A 56-year-old man was told by his wife that she wanted a divorce.
He made suicidal statements and left the house.
His wife called 911.
When the police arrived, they located him in the garage, lying under a blanket.
He had a calm demeanor and acknowledged that he had made suicidal statements.
He agreed to go to the ED for evaluation.
The police removed numerous guns from his house per the state’s red flag law.
In the ED, he spoke with the nurse and the ED physician.
He admitted to making suicidal statements, but reported that they were made in the heat of an argument and that he did not have any intent to kill himself.
The ED physician felt that the patient was honest and forthcoming during their discussion.
He felt that the patient was low-risk for suicide.
The patient was discharged without a psych consult.
No collateral information was obtained from his wife or other family members.
He subsequently died by suicide (no mechanism listed in any records).
An estate planning lawyer was appointed as the administrator of his estate.
A lawsuit was filed with 2 plaintiffs: the patient’s estate and the wife.
The ED physician unexpectedly passed away of cancer between the patient’s death and the lawsuit.
Therefore, the doctor’s wife was sued as the administrator of his estate.
The hospital and ED physician group were also named as defendants.
Join 15,000+ doctors and attorneys on the email list.
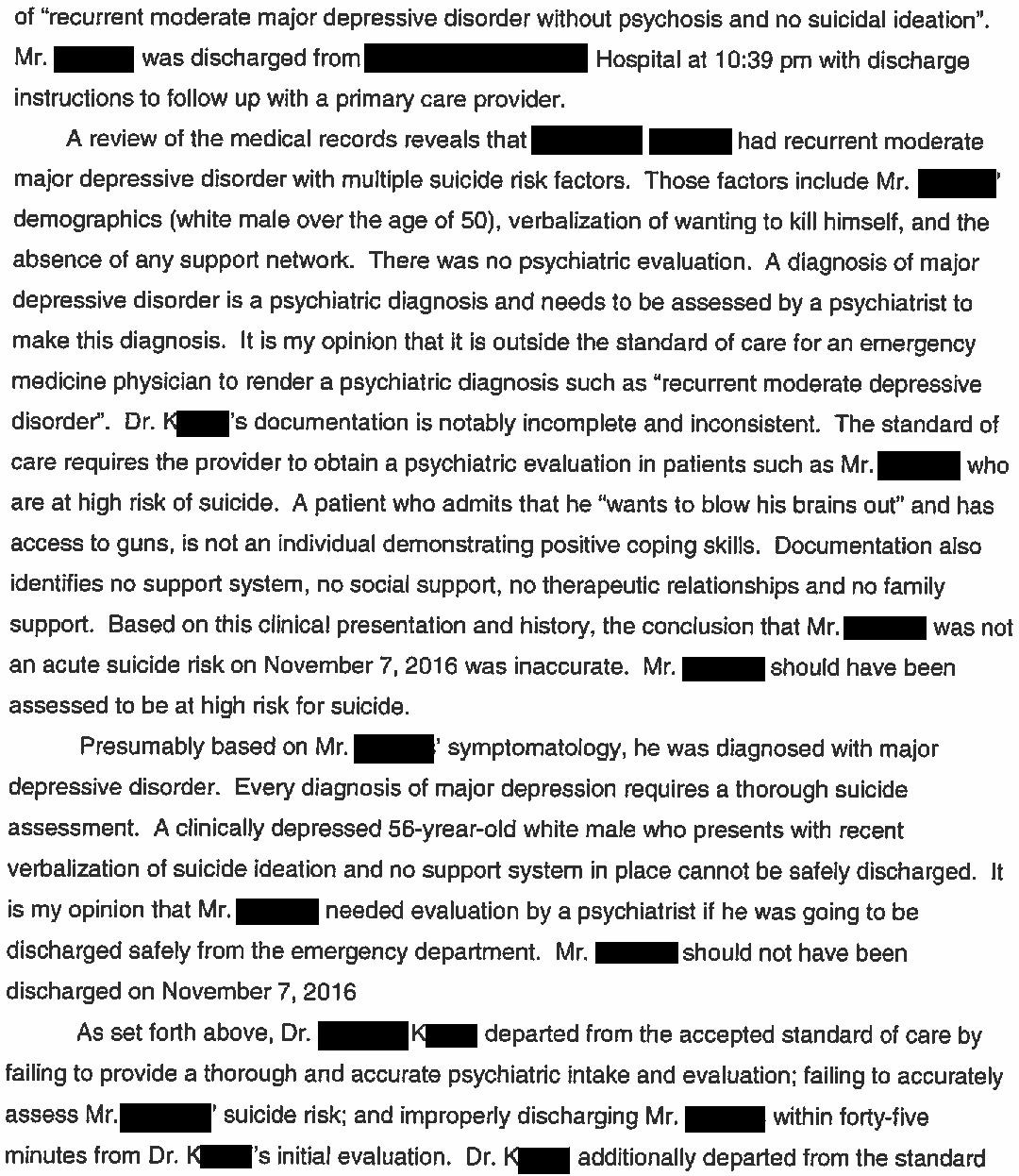
The plaintiff’s ED expert opinion is shown here:
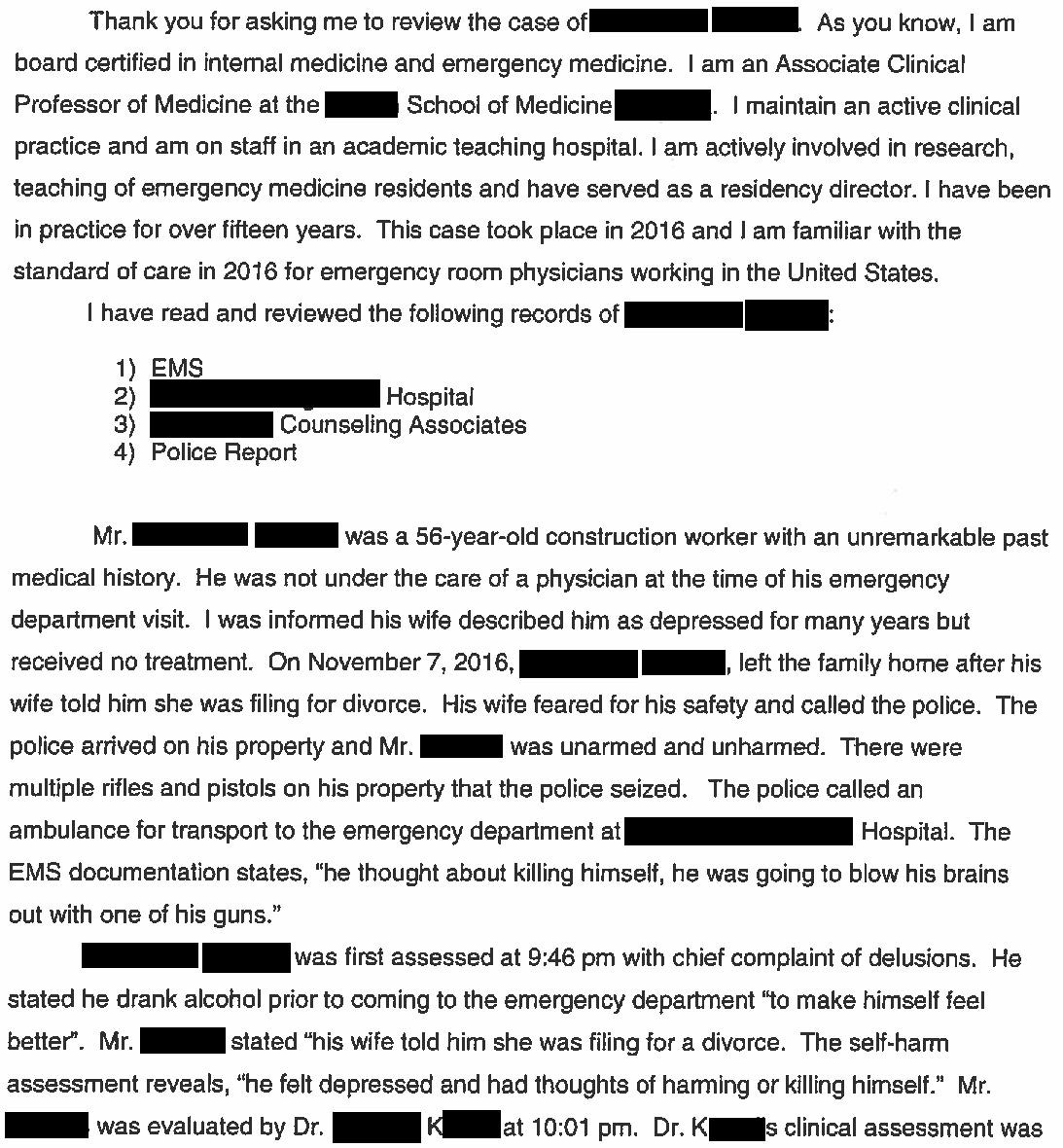
The plaintiffs offered to settle the case for $5,000,000.
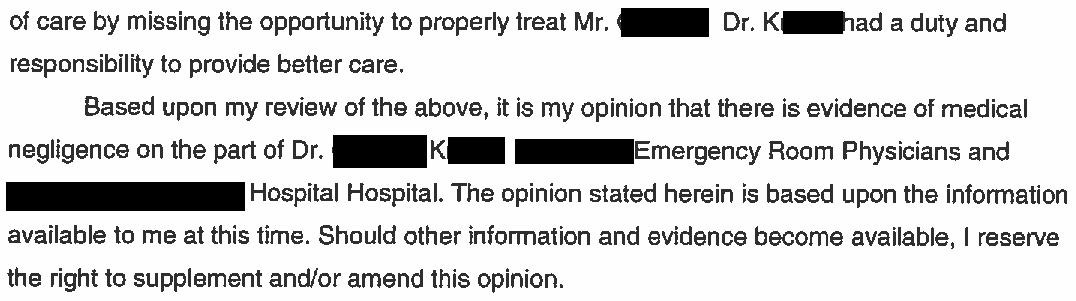
Further review of the court records indicate that the plaintiff’s expert left out numerous details that paint a more complicated picture.
The patient died 18 days after being seen in the ED.
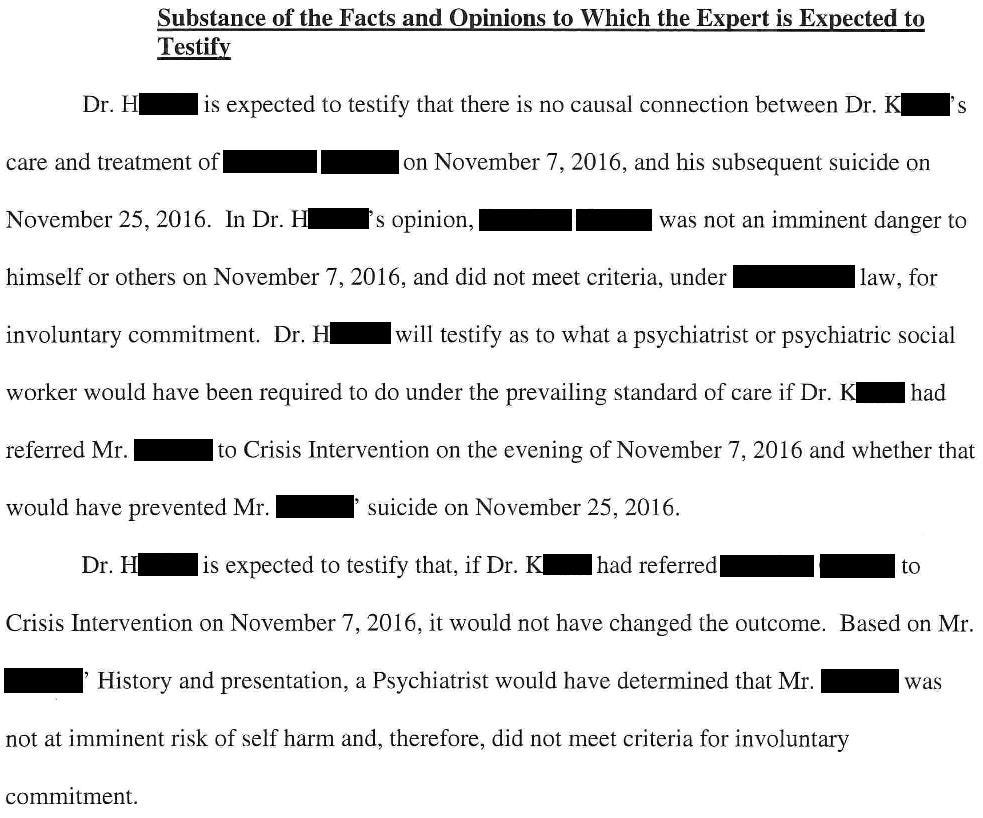
A psychiatry expert for the defense (actively practices emergency psychiatry and is the PD of a psychiatry residency program) highlighted this in his opinion:
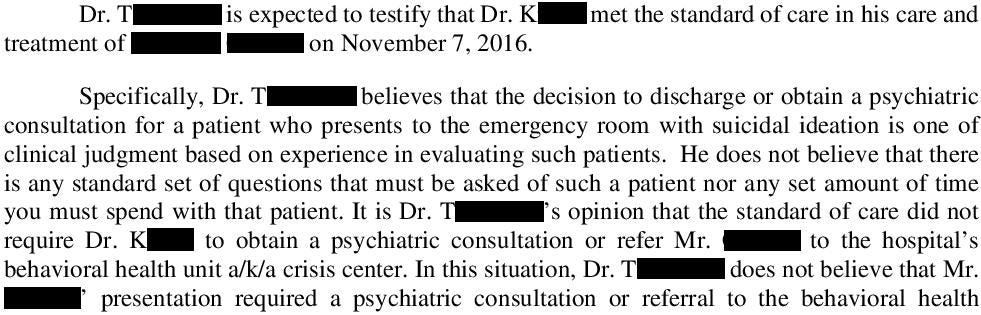
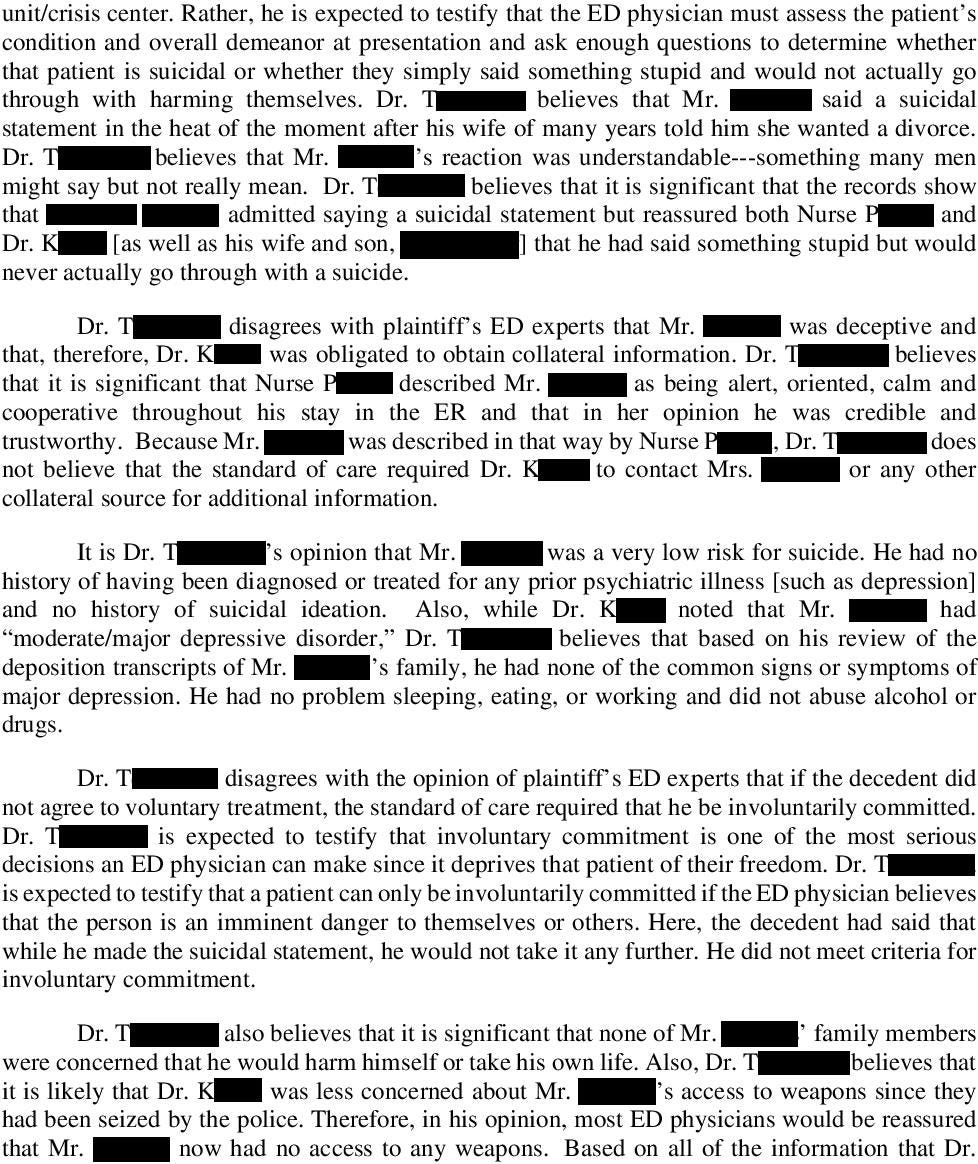
An EM expert for the defense wrote the following opinion:

Learn from malpractice cases without going through them yourself.
Become a medicolegal expert.
Paying subscribers get a new case every week.
In between the ED visit and his death, the patient and his wife had 2 visits with a marriage therapist.
The therapist did not conduct a suicide risk assessment at either visit.
The defense lawyers filed an “apportionment complaint” against the therapist, which added her as a defendant.
This approach is an attempt to have some of the potential damages redirected away from the hospital, ED group, and doctor’s estate.
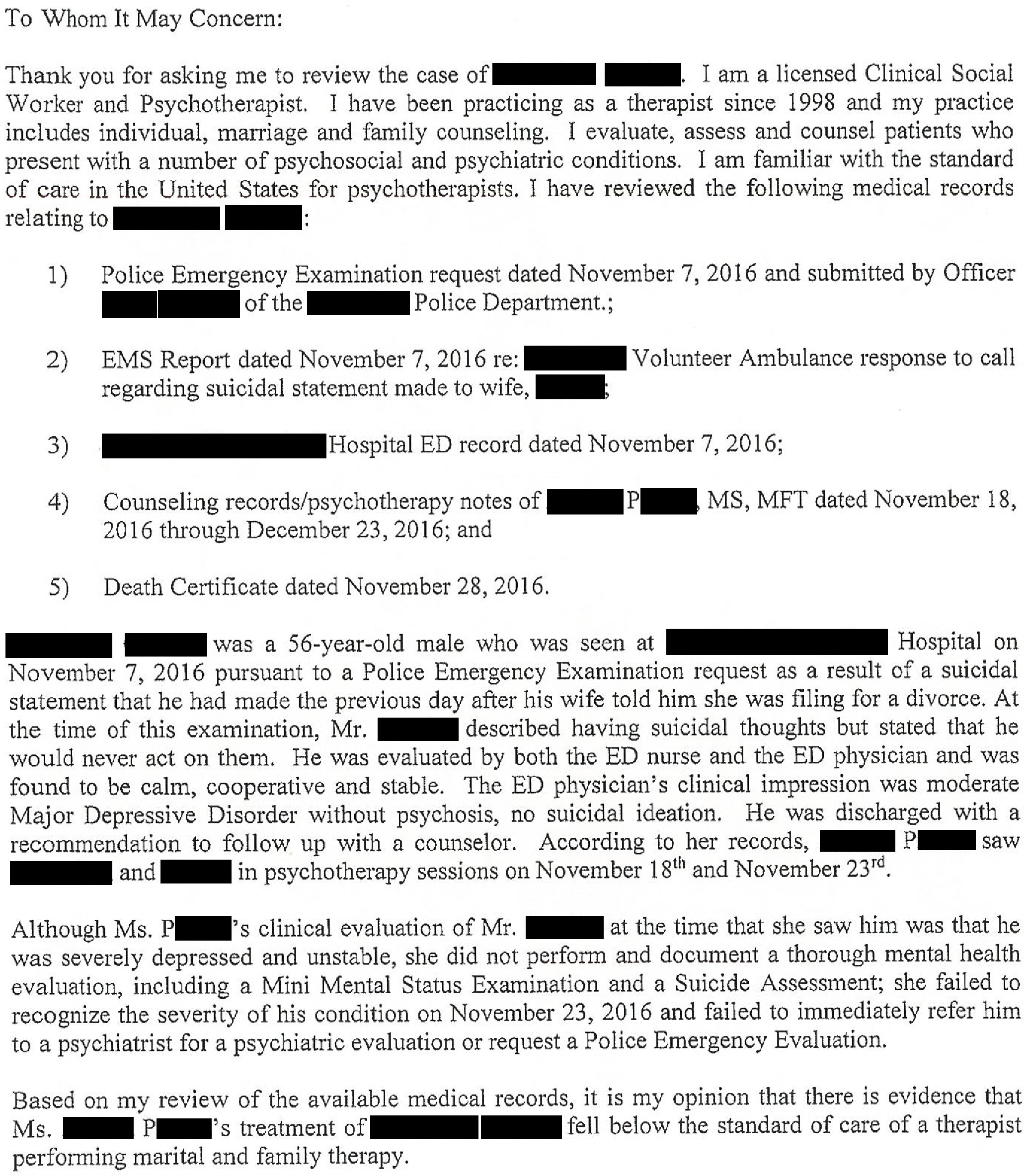
The defense hired a therapy expert:
During the defense attorney’s deposition of the patient’s wife, some new information surfaced.
Shortly before requesting a divorce, she had entered into a relationship with a different man.
The wife was adamant that at the time of the patient’s death, it was simply a friendship without any sexual overtones.
She noted that she and the other man joined another couple on camping trips and trips to a casino, and that her husband was unaware of this.
A few months after the patient’s death, she entered into a romantic relationship with the other man.
The plaintiffs filed a motion in limine, which (if granted by the judge) would prevent the defense from mentioning this relationship to the jury.
After this information came to light, the plaintiff’s attorney removed the patient’s wife as a plaintiff.
The lawsuit continued with a single plaintiff (the deceased patient’s estate).
An economics expert was named and wrote the following reports about the patient’s lost earning potential.
The first was based on one year (2014) of earnings, and assumed he would work until either age 67 or 70.
The second estimate used an average of the past few year’s income, as opposed to one year.
All of the remaining parties reached a confidential settlement before trial.
Update January 2, 2024:
I was able to obtain a copy of the death certificate.
It indicates the patient shot himself in the head with a shotgun:

MedMalReviewer Analysis:
In my opinion the ED doctor fell below the standard of care by not obtaining a psychiatry consult. Based on his numerous risk factors, there was a reasonably high chance of suicide. I’m confident that the vast, vast majority of ED doctors would consult psych on this patient. I think the doctor was lulled into complacency by the fact that the patient was speaking in a calm and controlled manner, openly acknowledged his previous suicidal statements, rationalized them as being made in the heat of the argument, and reassured the doctor that he wouldn’t actually do it. When a patient is brought to the ED for suicidal statements and is claiming they are no longer suicidal, its a much easier decision to place them on a hold if they’re highly emotional, screaming, denying that they ever made suicidal statements, and are not able to give a logical explanation for their change of mind.
Despite the ED doctor failing to meet the standard of care, I am not convinced that consulting psych and admitting him to the hospital against his will would have prevented his suicide 18 days later. But it’s impossible to know for certain. If he had died 2-3 days after the ED visit, the plaintiffs would have had a much better argument. If he had died a decade later, it obviously would not have been a result of negligence at the ED visit. The subacute timeframe really blurs the lines. What do you think?
The patient’s guns were removed from his home per the state’s red flag law. It did not stop his death. The records do not indicate if he had already been given his guns back. There’s not enough information here to draw a clear conclusion and even if we had all the details, policy should not be based on anecdotes.
The discovery of the wife’s relationship with another man really casts this lawsuit in a new light. It’s not my place to make unsubstantiated guesses about the true nature of their relationship, but it’s obvious that this information would have turned a jury of lay people against the plaintiff. They would have seen her as a cheater who caused her husband’s suicide, and now was trying to get rich by blaming someone else and suing them. I suspect the plaintiff’s attorney did not know about this relationship before the deposition. Why else would they remove her from the lawsuit after this came to light? I’d imagine her attorney was banging his head against a wall after walking out of the deposition.
The ED physician did not fall below the standard of care by not consulting a psychiatrist. Many places, mine included, psych will not see patients in the ED. This patient had the capacity to make his own decisions, was not demonstrating signs or symptoms of AMS/intox/psychosis, and was not in any imminent danger to himself or others. While sad this man took his life, the ED physician did not contribute to his death. I would like to see the RN and physician documentation to see how they justified their assessment and decision making.
If an individual is determined to take his life, they will. As a neurologist, I once cared for a comatose patient who it turned out had taken an overdose in a suicide attempt. He survived and was discharged to a psychiatric facility. After several days there, he was discharged to home and promptly killed himself. Also, a local psychiatrist was sued a number of years ago after his patient killed himself. The judge reversed a jury verdict against the doctor reasoning that the psychiatrist should not be expected to predict the future with certainty. Even in psychiatric facilities, suicides can and have taken place.