


Suicide by Hanging on Psych Floor
Case #237

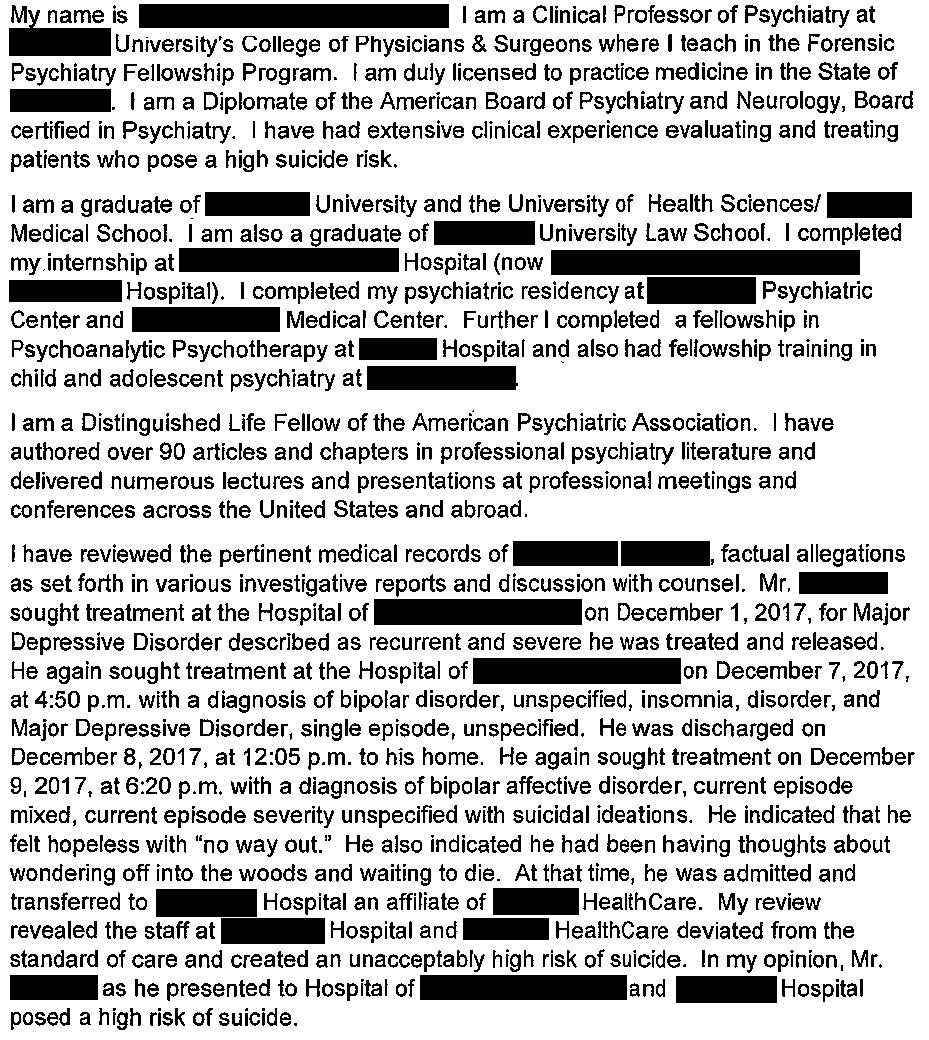
A 56-year-old man presented to the ED with vague suicidal ideation.
This was his 3rd visit for depression in the last 10 days.
He was admitted to the psych floor.
The patient was cooperative with therapy and medication changes.
He was checked every 15 minutes per the hospital’s protocol.
On day 6 of hospitalization, he was seen in the dining room around noon, then went back to his room.

Become a better doctor.
Paying subscribers get a new case every week and access to the entire archive.
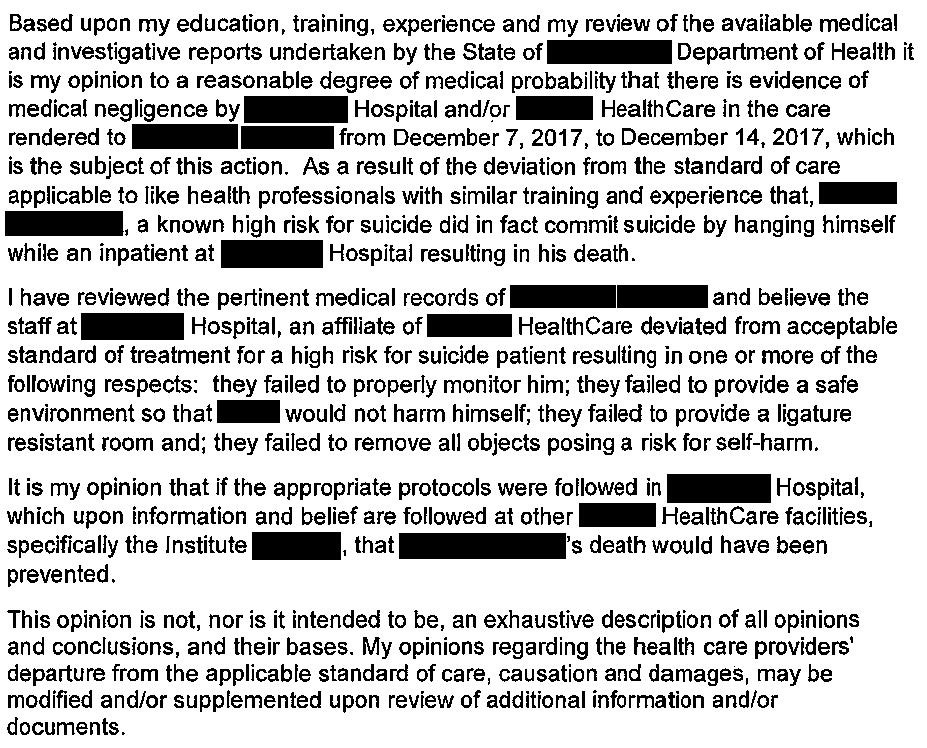
The patient’s brother filed a lawsuit against the hospital and the psychiatrist.
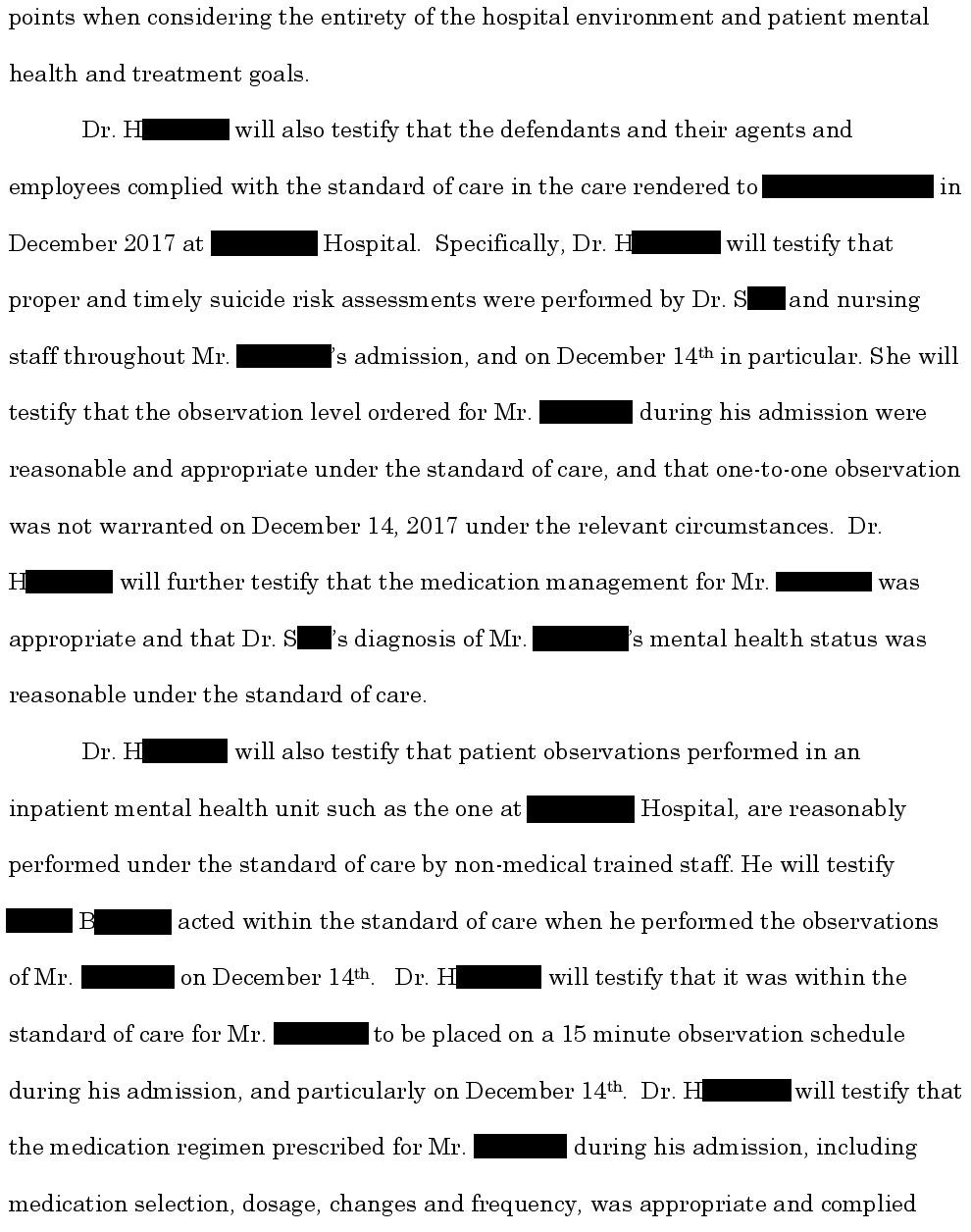
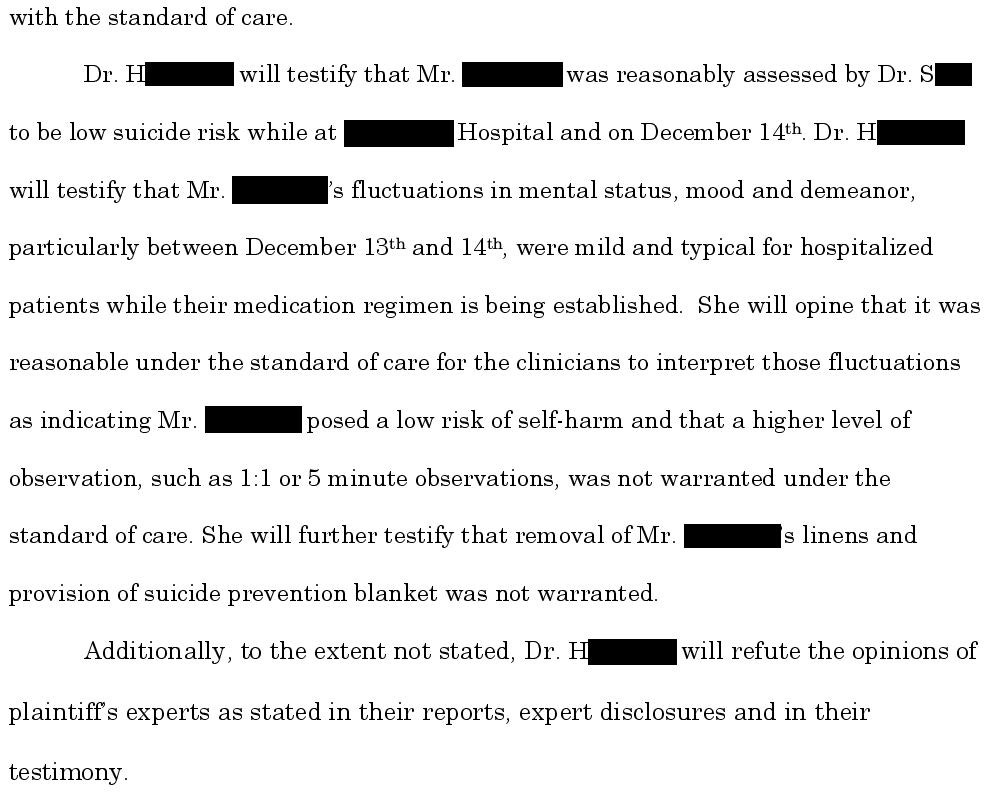
The expert witness opinion is shown here:
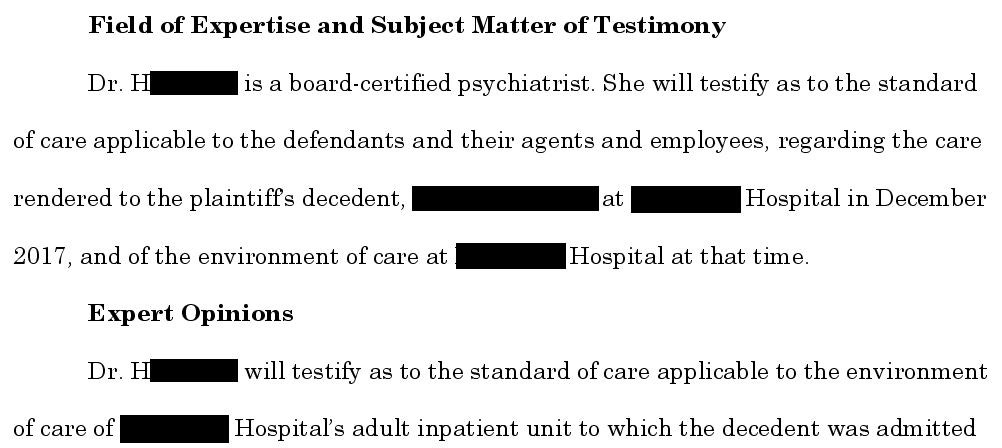
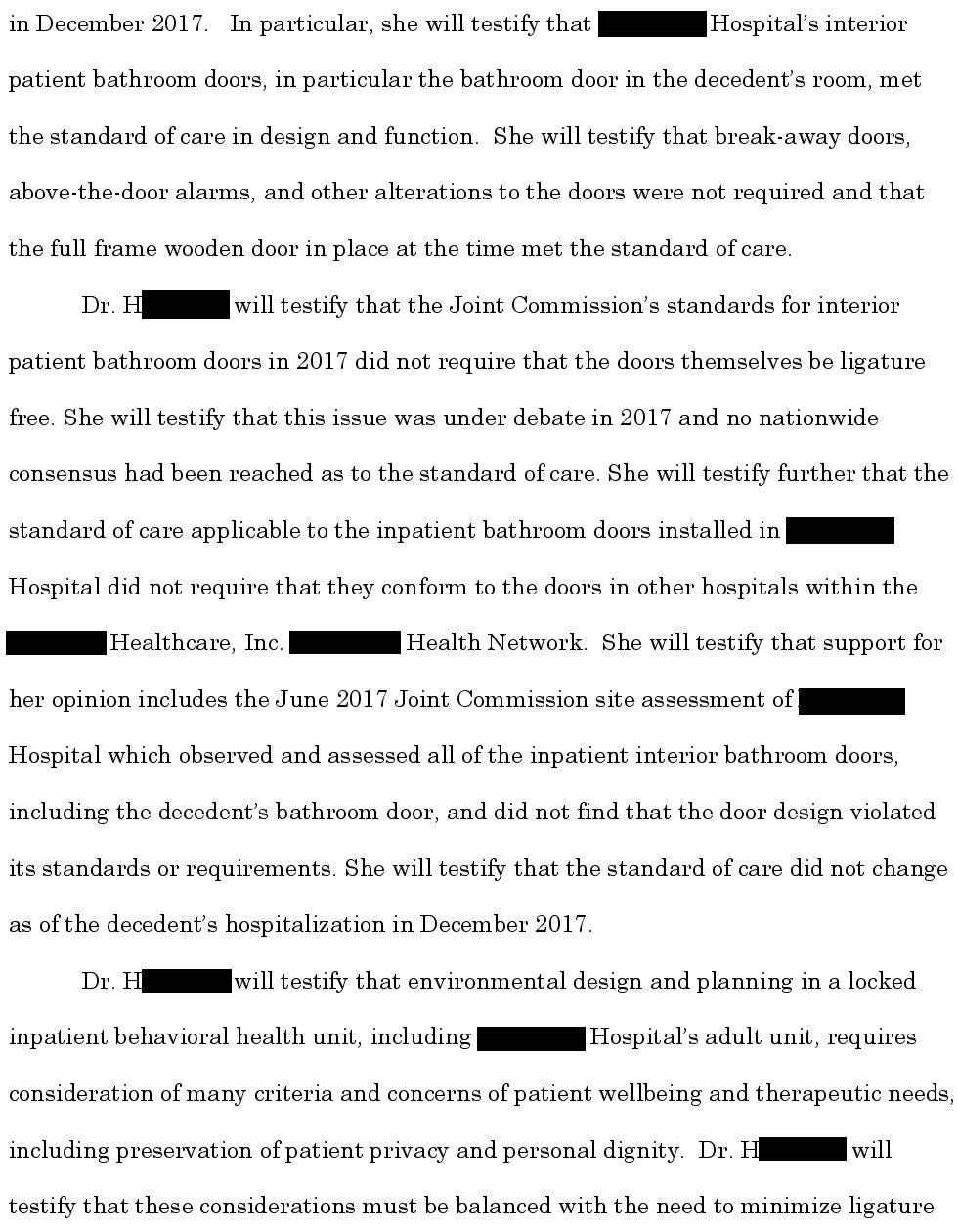
The defense hired their own psychiatrist.
Protect yourself from lawsuits through weekly case review.
Expand your medicolegal expertise by reading cases and identifying common themes.
The patient’s brother was deposed and indicated he had a life insurance policy.

The plaintiff offered to settle the lawsuit for $3,000,000.

The lawsuit is ongoing.
Signed up for the email list to be notified about the conclusion.
MedMalReviewer Analysis:
The points about ligature-resistant rooms would be best addressed by a hospital design expert rather than a physician. Physicians should be involved with the design of hospitals but each individual physician showing up to work in a building that was constructed long before they were hired shouldn’t shoulder any responsibility for environmental issues. These accusations are included by the plaintiff to hold the hospital liable, rather than the individual physician.
The physician is responsible for determining the level of observation for a patient (q15 minute checks vs q5 minute vs constant observation). There’s nothing in this case to suggest that constant observation was necessary. His suicidal thoughts seems vague and more in line with a passive death wish than an active plan (“wandering off into the woods and waiting to die”). From the information provided, I agree with the defense expert and defendant’s assessment that he was low risk.
I’ve published multiple previous suicide malpractice cases. This is the second one I’ve covered regarding suicide while in a psych facility (the previous one is linked below). Admitting patients to an inpatient psych facility may be beneficial, but doesn’t absolutely guarantee their safety.

I’m always interested in reflecting upon the relationship between the medical care we provide and the research/studies that support that care. We like to think we are strictly evidence-based, but there are numerous decisions we make that are unsupported by high quality evidence. As far as I’m aware, there are no RCTs to suggest that admitting suicidal patients reduces the likelihood of suicide (please leave a link in the comments if I’ve missed one). There would be vigorous debate as to the ethics of such a study, but it’s worth acknowledging the reality of the literature we have.
First, I acknowledge the horror we feel at the death of a person by PROXIMATE action. This is what we commonly call Suicide (self-death, for the Latin survivors.) I've seen plenty and enough. These are likely not truly preventable by physicians as much as we like to self-aggrandize. Witness the increase in suicides despite increasing mental health outreach. This is likely a societal problem about which we can advise but not fix. "Deaths of despair" are not amenable to our ministrations. (This is another whole discussion, I recommend Viktor Frankl and Albert Camus. Read them then come back.)
Strangely, we don't feel the revulsion/reaction at the much more common self-killing: tobacco, alcohol, poor life choices. Instead, we "blame the victim." The only difference is proximity, not cause.
In my not-very-humble opinion, we need a little more humility. We need to start a discussion on self-determination and respect for self-determination.. This absolutely does not mean we abandon the high position of seeing, advising and treating people wanting help. However, we need to acknowledge that, unless we are willing to take these patients home with us, live in our homes, use our bathrooms and kitchens, we have limited (at best) control over the outcomes.
The right of self-determination and, ultimately, knowingly taking responsibility for the consequences (whatever they be: refuse vaccination and accept the disease the the transmission thereof, jaywalk irresponsibly, smoke, use substances, not take prescribed meds, etc., etc.) is, in the end, respect for the individual.
We, as a profession, need to have a hard discussion.
Very much agree with Thomas above.
I was just talking with a resident last night about how difficult suicide risk stratification is and therefore how difficult it is to teach. The evidence for specific risk factors is murky at best, the evidence that any of our interventions are particularly effective is probably worse, and the patients who are the highest risk are not going to seek help and are going to obfuscate if forced to do so.
All this leads to a situation where your actual risk assessment is largely based on vibes and everything else is just trying to protect yourself legally. And unfortunately we've created a system where there is strong incentive to take patients' rights away in a way that can follow them for life in order to administer questionably effective treatment just to cover ourselves from liability.