



A 53-year-old man developed mild dysphagia.
Workup revealed a mediastinal mass and biopsies were done.
He was diagnosed with Hodgkin lymphoma.
He was referred to an oncologist (Dr. G).
Dr. G recommended 2 cycles of chemotherapy (ABVD: adriamycin, bleomycin, vinblastine, dacarbazine), then reassessment to decide on the next steps.
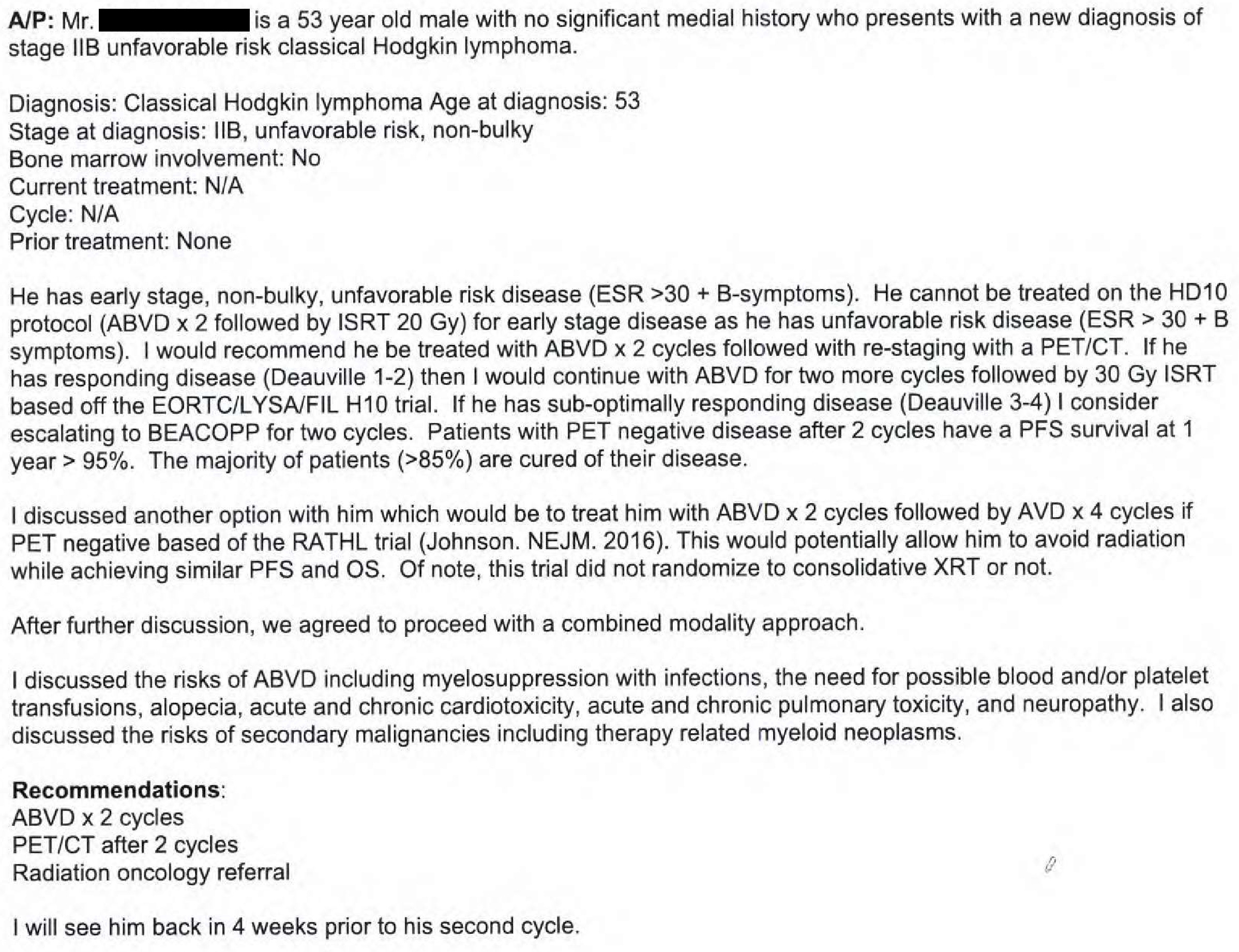
Note that he specifically discussed the risks of ABVD, including the possibility of bleomycin-related pulmonary toxicity.
Join thousands of doctors on the email list:
Following both cycles of ABVD, he had a follow-up appointment with Dr. G on November 29.
He had an excellent response, so 2 more cycles of ABVD were ordered.
The patient had mild dyspnea on exertion.
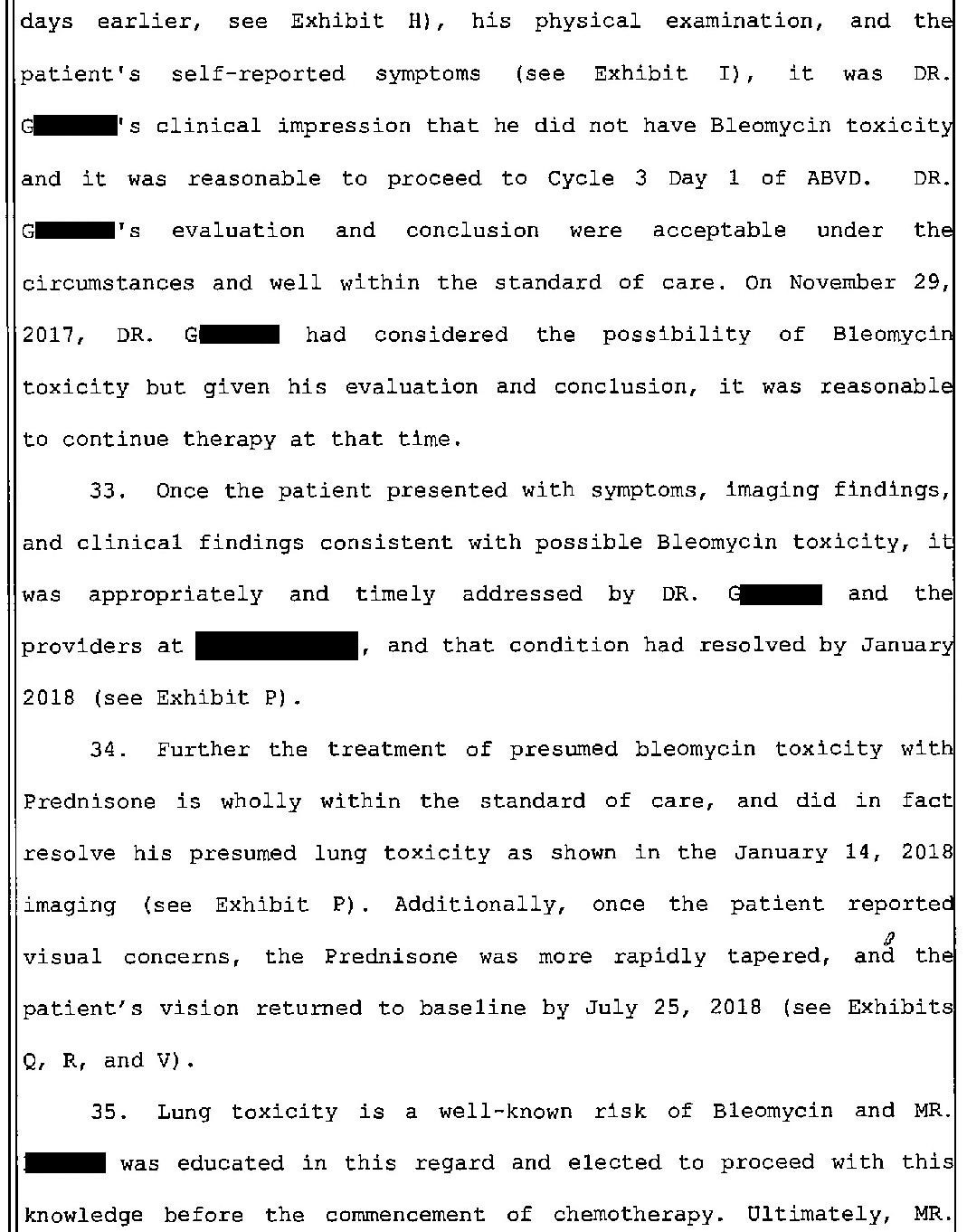
However, he had clear lungs on exam and his O2 sat was 98% on room air so Dr. G did not feel this was bleomycin toxicity and did not start steroids.

The patient would later accuse Dr. G of negligence based on the fact that he did not diagnose bleomycin pulmonary toxicity at this visit.
Cycle 3 was delayed for several days due to concern for bleomycin toxicity.
He remained slightly dyspneic.
However, he passed a road test without any hypoxia and cycle 3 was given.
A week after cycle 3, he developed a fever and went to the ED.
Imaging showed pulmonary consolidations, and he was still dyspneic.
It was unclear if the pulmonary findings were due to pneumonia or bleomycin toxicity, therefore both antibiotics and steroids were ordered.
The inpatient oncology team was consulted.

The patient followed-up with Dr. G after he was discharged.
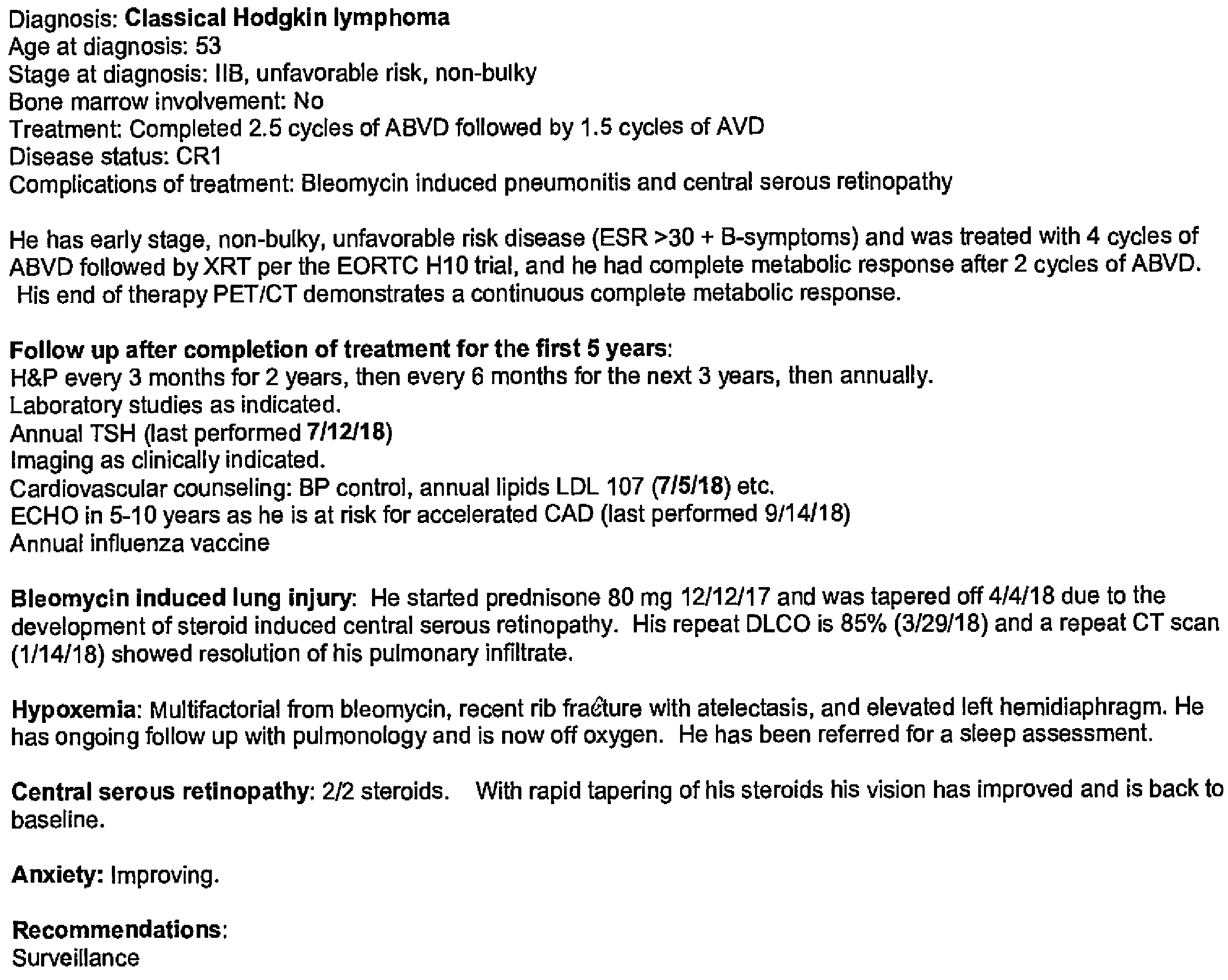
He elected to discontinue bleomycin.
The patient was continued on the prednisone that was started during his admission, with a plan to taper it over 4 months.

His respiratory status improved on steroids.
His dyspnea resolved.
However, one month into the prednisone taper, he developed vision problems.
He called Dr. G’s office, and a next-day ophthalmology appointment was arranged.

The ophthalmologist diagnosed central serous retinopathy due to steroids.
Dr. G and the ophthalmologist decided to taper the patient’s steroids more rapidly.
The patient’s vision returned to normal.
His dyspnea resolved and he no longer required oxygen.
Most importantly, he cancer was successfully treated.
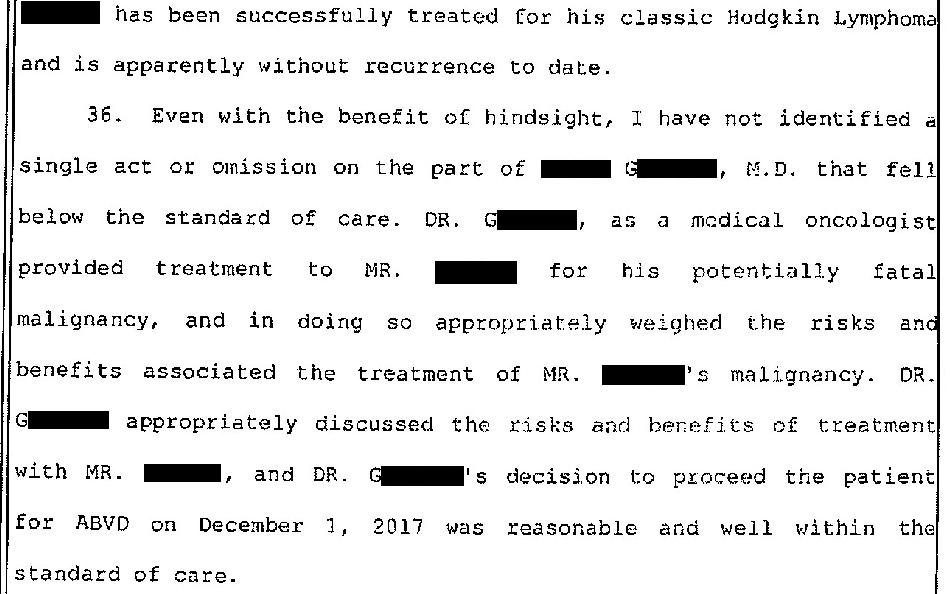
The note from Dr. G’s last visit is shown below.
"I always enjoy reading these and find them applicable to my practice as a hospitalist."
"Thanks for all the work you do in putting these together. Always so interesting to look at cases and see how things unfold. The cases also make great teaching points for the residents on rounds." - Dr. Emily Rushing
Despite the resolution of hypoxia, the patient claims to have been permanently disabled from bleomycin toxicity.
He consulted a lawyer and a lawsuit was filed against Dr. G.

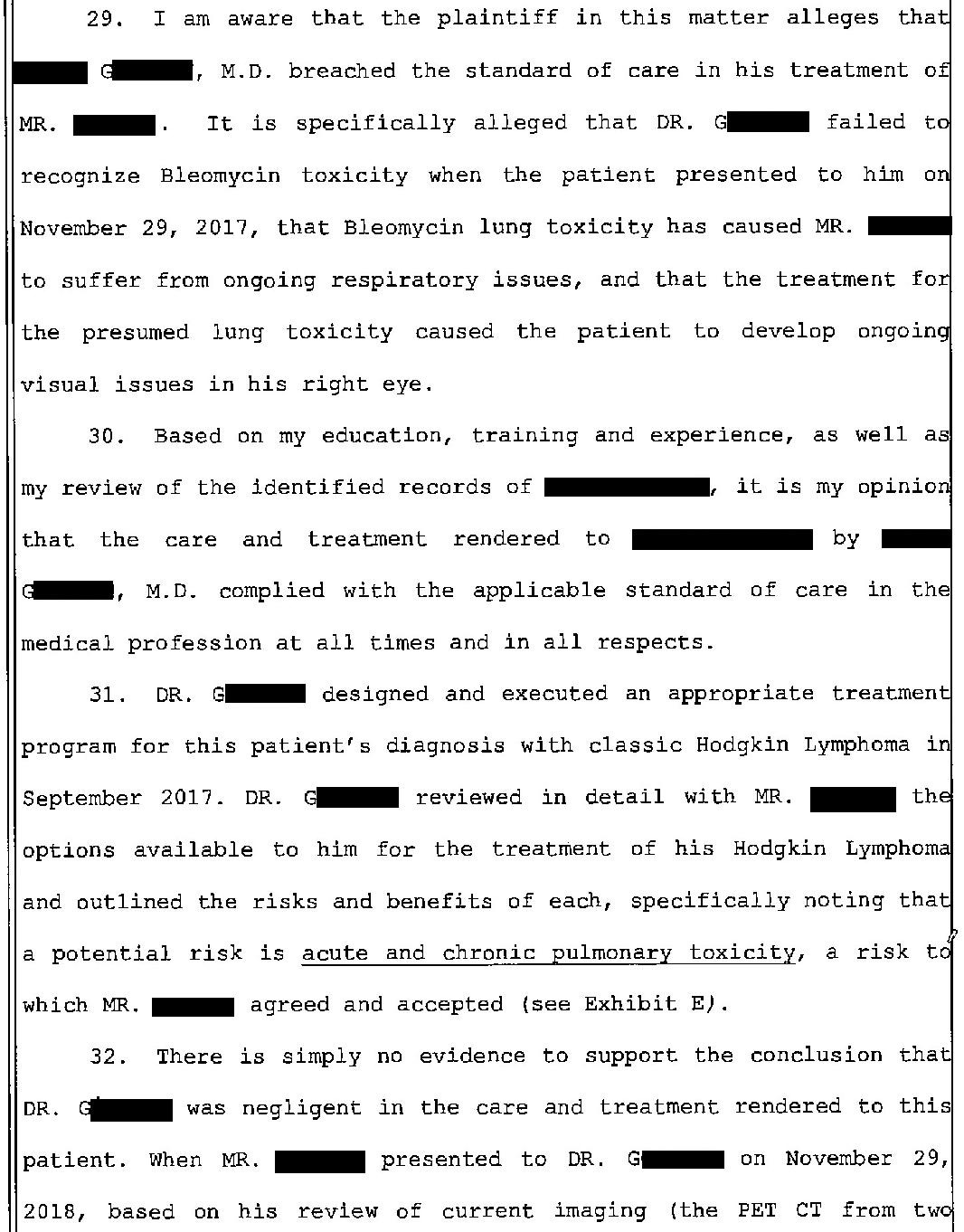
The defense hired an expert witness to review the case.
His conclusions are shown here:
The lawsuit played out over several years.
Dr. G vigorously denied any wrongdoing.
The day before trial, the plaintiff dropped the case.
A very small settlement was paid that only covered the plaintiff’s attorney’s costs.
It seems that they were trying to extract a settlement but knew they had a very weak case and would not prevail at trial.
The defense called their bluff.
MedMalReviewer Analysis:
This is as close to a frivolous lawsuit as I’ve seen. A patient was cured of his cancer and then sued over minor and reversible side effects that he was warned about and for which he was closely monitored. I can’t think of a more rude and ungrateful response to someone who saved your life. Lawsuits like these cause enmity between doctors and patients, drive up the costs of healthcare, and are an embarrassment to the plaintiff’s bar.
This is an excellent case series and review of pulmonary toxicity from bleomycin. It’s worth reviewing for generalists (especially ED physicians, hospitalists and primary care physicians) who may not encounter these patients frequently.
The importance of good documentation is highlighted in this case. Dr. G clearly documented the discussion of risks, including the most common side effects (specifically mentioning “acute and chronic pulmonary toxicity”). This example drives home a key learning point about documentation and malpractice: Good documentation will not prevent a lawsuit, but it goes a long way in helping your legal team mount a successful defense.
Recent Cases:
Testicular Ischemia After Hernia Repair [Paying Subscribers Only]
Thoracic Aortic Aneurysm Misdiagnosed as Endocarditis
Oncologist Fails to Follow-Up on Lung Nodule [Paying Subscribers Only]
I think MMR's first point hits the nail on the head. This is one of the most asinine malpractice claims I've ever seen. I can't believe the plaintiff even got attorney's fees. Would love to see what fault the plaintiff's "expert" supposedly saw in the care here.
So, what I take from this is that a doctor can provide outstanding, evidence-based care, attentive follow up, excellent documentation, and save someone's life from a deadly malignancy, and their thanks at the end of the day is a lawsuit.
Especially disappointing considering how clear it is that Dr. G was eminently knowledgeable, cared about this patient, steered through the curveballs, and saved a man's life. These are some fantastic examples of excellent clinical documentation. Everything about Dr. G's thought process was crystal clear, and a plaintiff's attorney would have to turn themselves inside out trying to impeach it at trial. Even if Dr. G "missed" bleo toxicity (for the sake of argument), there is an abundantly clear demonstration from his notes that he considered the possibility, assessed for it, and made a reasonable argument from his assessment why no further workup was needed. That's so far removed from the realm of "negligence," I have to know what the plaintiff's "expert" was smoking when they reviewed this case.
How incredibly entitled for someone to go after their physician after getting their cancer cured. If his cancer ever recurs, he may regret having blacklisted himself from that practice. Good on the MD for not settling but I wish we had more protections about blatant frivolous cases. At least the plaintiff should be stuck with his own lawyer fees.