


Death After ED Visit for COVID
Case #271

A 21-year-old college student went to the ED for cough, chest pain, and shortness of breath.
He had been diagnosed with COVID at an urgent care 3 days earlier.
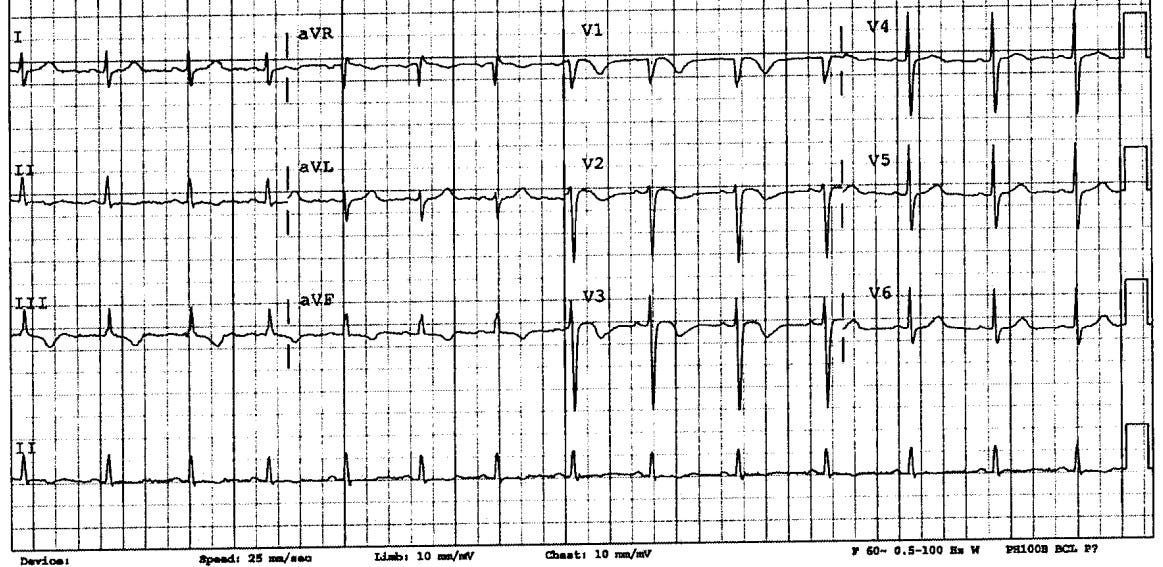
An EKG was done.
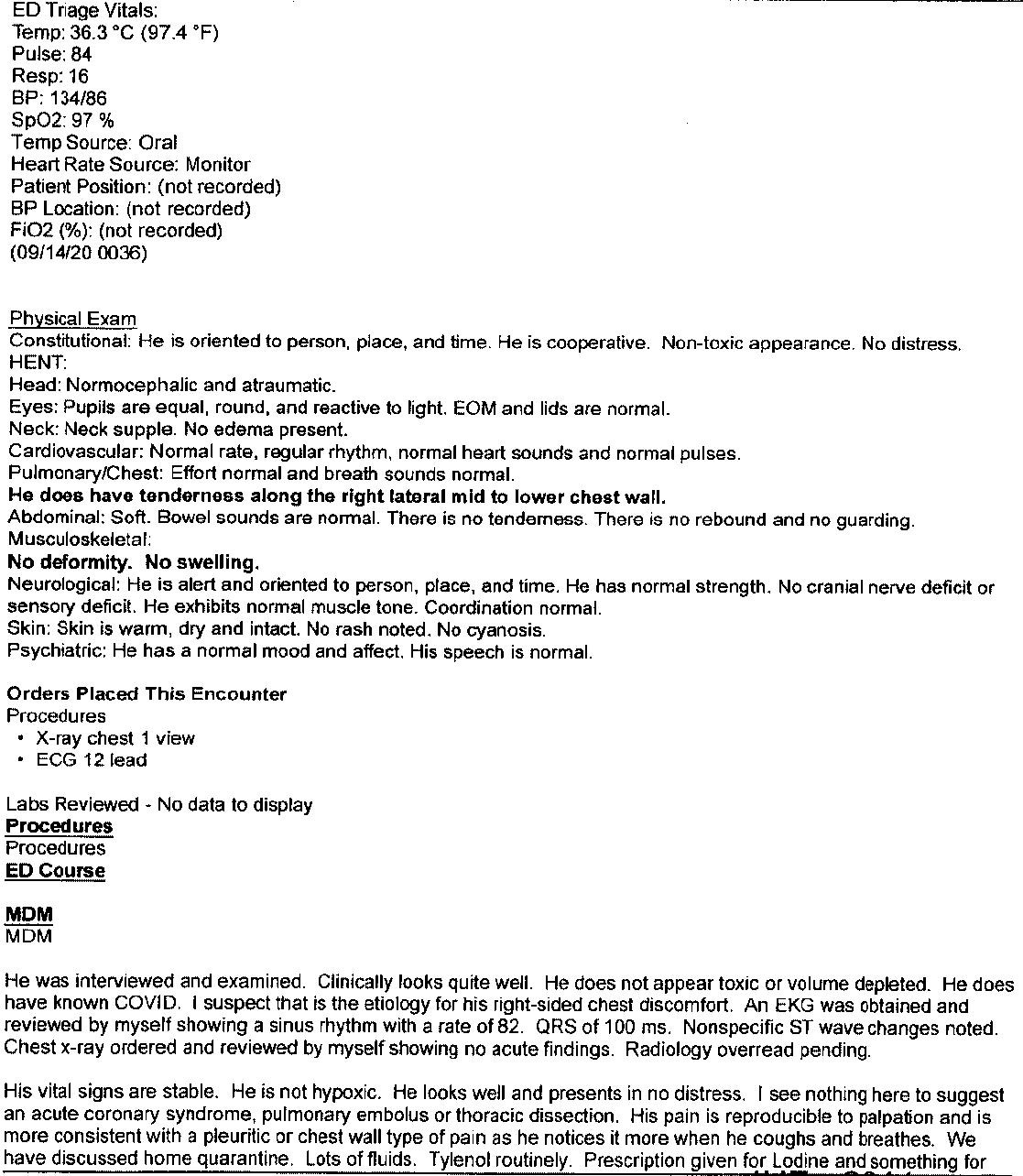
The ED note is shown below:
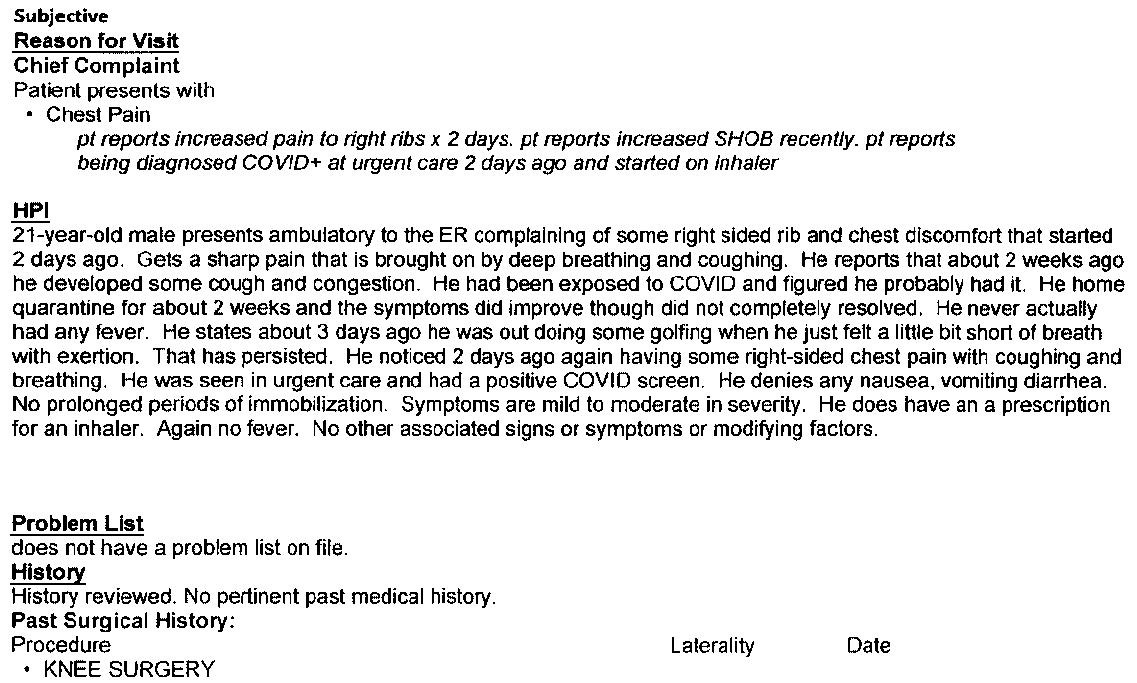

Become a better doctor by reviewing med mal cases.
Subscribe today to get a new case every week.
The patient returned home.
Over the next week he continued to have symptoms.
A week after the ED visit, he had a syncopal episode while running up stairs.
EMS was called but he declined transport to the hospital.
The patient’s friends would later claim that the EMS crew told him he would be fine and pressured him to sign the refusal form.
6 days after the EMS visit, the patient had a cardiac arrest.
EMS obtained ROSC and he was taken to the ED.
The patient was diagnosed with massive pulmonary emboli and admitted to the ICU.
Neurologic function did not return.
He died 5 days after the cardiac arrest.
The patient’s parents filed a lawsuit against the ED physician and hospital.
They did not sue the urgent care nor the EMS service.
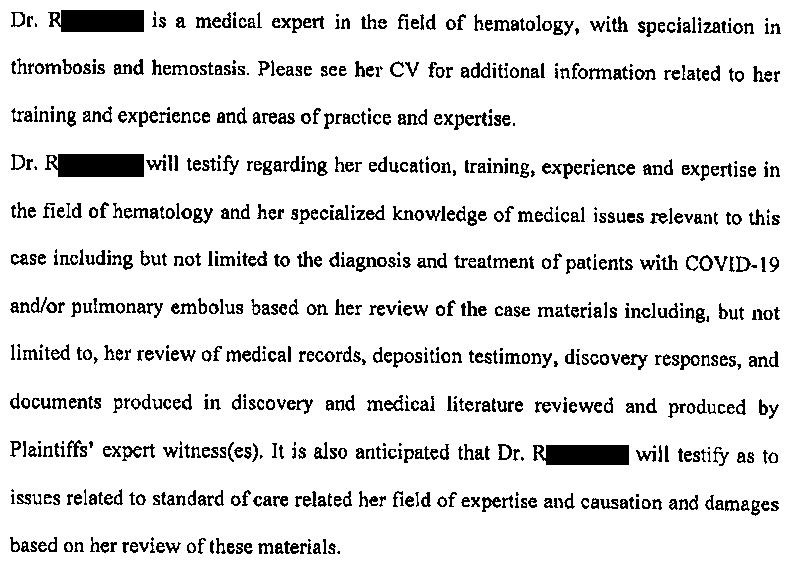
Multiple expert witnesses were hired including ED, cardiology, and hematology.
The only written expert report included in the court records was a hematologist for the defense.
The state in which this happened had a COVID-19 Limited Liability Act that was in force at the time of this case.
The relevant part of the law is shown below.
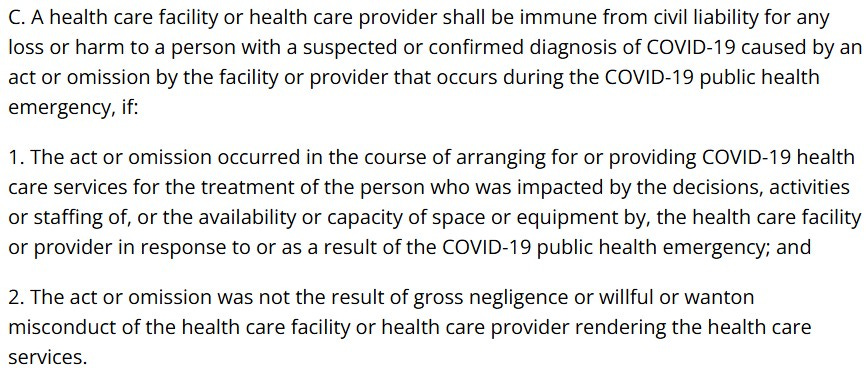
The defense felt that the Limited Liability Act applied to this case, and asked that the lawsuit be thrown out.
The plaintiff felt that the pandemic did not influence the testing that could have been done, and therefore the law did not apply to this case.
They also cited their EM and cardiology experts, who claimed that the failure to order additional testing after reviewing the EKG met the definition of gross negligence.
Gross negligence has been defined in this state’s law and by their Supreme Court in various ways:
“the want [lack] of slight care and diligence”
conduct that is “so flagrant, so deliberate, or so reckless that it is removed from the realm of mere negligence.”
“reckless indifference to the consequences”
The judge refused to throw the lawsuit out, and decided it would be up to the jury to decide if the Limited Liability Act would apply in this case.
The two sides were unable to reach a settlement before trial.
The jury decided that the Limited Liability Act did not apply in this case.
They returned a $10,000,000 verdict against the doctor and hospital.
They assigned 25% of the blame to the deceased patient.

The verdict is currently being appealed.
Improve your practice and learn from challenging cases.
Subscribe today.
CME credit available.
MedMalReviewer Analysis:
This case is an undeniable tragedy. I watched a memorial video made by the patient’s mother and it was heart-wrenching. That being said, a medical malpractice lawsuit should not be decided based on emotion. In my opinion, it was reasonable for the doctor to attribute cough, chest pain, and shortness of breath to COVID. The patient did not have any of the usual findings that would suggest PE such as tachycardia, hypoxia, or leg swelling, and did not report any PE risk factors (although may have had a family history of antithrombin III deficiency that was unreported). If there is concern for PE, the appropriate workup starts with risk stratification (Wells, modified Geneva, or clinician gestalt). This patient’s modified Geneva score is zero, and therefore he is low risk for PE. Low risk patients are eligible for PERC. This patient “PERCs out” and therefore there is no indication for d-dimer or CT. The doctor didn’t document this thought process, but the fact remains that he followed the appropriate workup and met the standard of care.
The key issue in this case was whether the EKG should have triggered further workup despite his PERC-negative status. The doctor described the EKG as “nonspecific ST changes”. When I looked at it I noticed the inverted T waves in chest leads and inferiorly, but did not understand the significance of this pattern. After doing a lot of reading, I now feel that the key learning point from this case is recognizing that simultaneous T-wave inversions in V1 and III is associated with PE. The best articles about this pattern come from Dr. Smith’s ECG blog, where he cites 2 papers by Kosuge and Witting.
Kosuge wrote the original paper that described this association. They looked at patients with inverted precordial T waves who were ultimately diagnosed with PE or ACS. They found that a negative T wave in both V1 and III is highly suggestive of PE as opposed to ACS. Only 1% of patients with ACS had this finding, versus 88% of PE patients. They only looked at patients who had TWI in precordial leads AND were subsequently diagnosed with ACS or PE (among some other criteria that are beyond the scope of this blog) so this does not necessarily generalize to undifferentiated ED patients, but the fact that it had such strong test characteristics (97% PPV and 95% NPV) means you shouldn’t ignore this.
Witting did a study that is a better reflection of undifferentiated ED patients, looking at patients that were ultimately diagnosed with PE, ACS, or non-cardiac chest pain. They found >1mm T-wave inversions in both V1 and III in 11.3% of PE patients, 4.5% of ACS patients, and 4.8% of non-cardiac chest pain patients. These results reflect a much greater degree of ambiguity than the Kosuge study and explain why this EKG finding may not raise alarm bells in the real world. However, they found that >2mm TWI in V1, V2, III, aVF were found in 4% of PE cases, but was never found in patients with ACS or non-cardiac chest pain. I was fairly surprised to find this buried in Table 1 because the classical teaching is that there are no EKG findings that are pathognomonic for PE. And yet, this paper suggests that this long-held dogma is incorrect and there may actually be a pathognomonic EKG finding for PE (>2mm TWI in all 4 of these leads). I’m not quite willing to make a claim this bold (after all, only 4 patients met this criteria) but I think it deserves more publicity than it has gotten. Notably, I think the EKG in this case reflects this potentially-pathognomonic finding. The millimeter markings were lost on the court copy and it’s very close to being 2mm in aVF, but I think it’s there.
Steve Smith’s ECG blog has published tons of real-life cases about this exact same pattern (TWI in V1 and III indicating PE). They’re a bit easier to read than the 2 research papers above. I strongly recommend that you read this case from his blog and look through the links at the bottom… there’s over 20 PE cases that have this pattern. Note that while TWI in V1 and III raises the possibility that there may be a PE, it can also be found in patients who are hypoxic or have other respiratory pathology.
I’m sure that a few astute readers are familiar with this pattern, but I doubt the majority of doctors are familiar with it’s specific description and association with PE. It was first described in 2006 and is slowly gaining more attention. I think any of us would be very worried about this EKG if it was an elderly patient with acute chest pain and history of coronary artery disease, but in a young man with COVID, I can see how it might not prompt further workup. Furthermore, the patient did not have the more commonly taught EKG findings including sinus tachycardia or S1Q3T3.
This is the benefit of reviewing med mal cases… it allows us to hammer home rare learning pearls in a way that is absolutely unforgettable. If you read about this topic in a boring journal article, you’ll probably forget it. If you read about it in the context of a dead college student and a doctor who lost a $10,000,000 verdict, it’s unforgettable.
With the benefit of hindsight, there are 2 other issues that could have raised concern and triggered a bigger workup:
The timeline didn’t make sense for COVID. The patient described 2 weeks of symptoms of cough and congestion. However, it wasn’t until the last few days that he developed shortness of breath with exertion and chest pain. These new symptoms represent a departure from the expected clinical COVID course. I would expect a healthy young man to be feeling better by that point, not developing new symptoms that are more concerning.
This patient had gone to an urgent care a few days earlier, and now had come to an ED. Many physicians will do a bigger workup than usual if a patient is a bounceback (although this is extremely context-specific and not the standard of care). The doctor did choose to do a bigger workup than urgent care (CXR and EKG), but no lab testing. ED doctors get criticized for ordering troponins and dimers too often, but it may have saved this patient’s life.
I’m surprised that the EMS crew wasn’t named in this lawsuit as well. Their note and the signed refusal form provide a vigorous defense, but the testimony from multiple witnesses was that there was pressure to refuse care. It’s impossible to say if this really happened or is self-serving testimony. I’m not arguing that the EMS crew really did put pressure on him to refuse, but the fact that this was exertional syncope should raise more concern than the standard vasovagal or orthostatic syncope that EMS responds to numerous times per day. I think the plaintiff’s attorney realized that the case against the EMS crew would be hard to prove with such good documentation, and that the potential financial benefits were slim.
I’m worried that the jury was overly harsh on the defendants because they attempted to use the COVID law to avoid liability. There is already a massive public backlash against the way the pandemic was handled, and it’s likely that some jury members harbored hypercritical views about this topic. They may have seen this as their chance to hold authority figures accountable. I wonder if it would be a better defense tactic to only use the COVID laws during pre-trial attempts to have the lawsuit thrown out, but if the judge refuses to dismiss it, purposefully do not use it as an argument in front of the jury. This case happened in a very conservative state. Before everyone gets political in the comment section, I will note that the last lawsuit I published that involved the defense unsuccessfully trying to avoid liability due to COVID laws happened in a very liberal state. If these 2 cases are reflective of a larger trend, it does not seem that these COVID laws actually provided much protection and only gave healthcare workers false reassurance.
Ten million dollars for a death of a young person with presumably no dependents? No amount of money will bring this person back and while the parents have suffered, funding their retirement is not the answer. The health care system simply can’t afford to hand out sums of money like this. I am glad to practice in a state where there are limits in non economic damages.
It is extremely scary for me as a resident. We’re always taught about EBM, and it’s unfortunate that Wells, PERC and Geneva all place patient as low risk and don’t account for ECG changes and yet still
the ED provider was found liable. I find this very curious that we can still follow EBM and be found liable