


Antibiotic Mismanagement Causes Renal Failure
Case #243

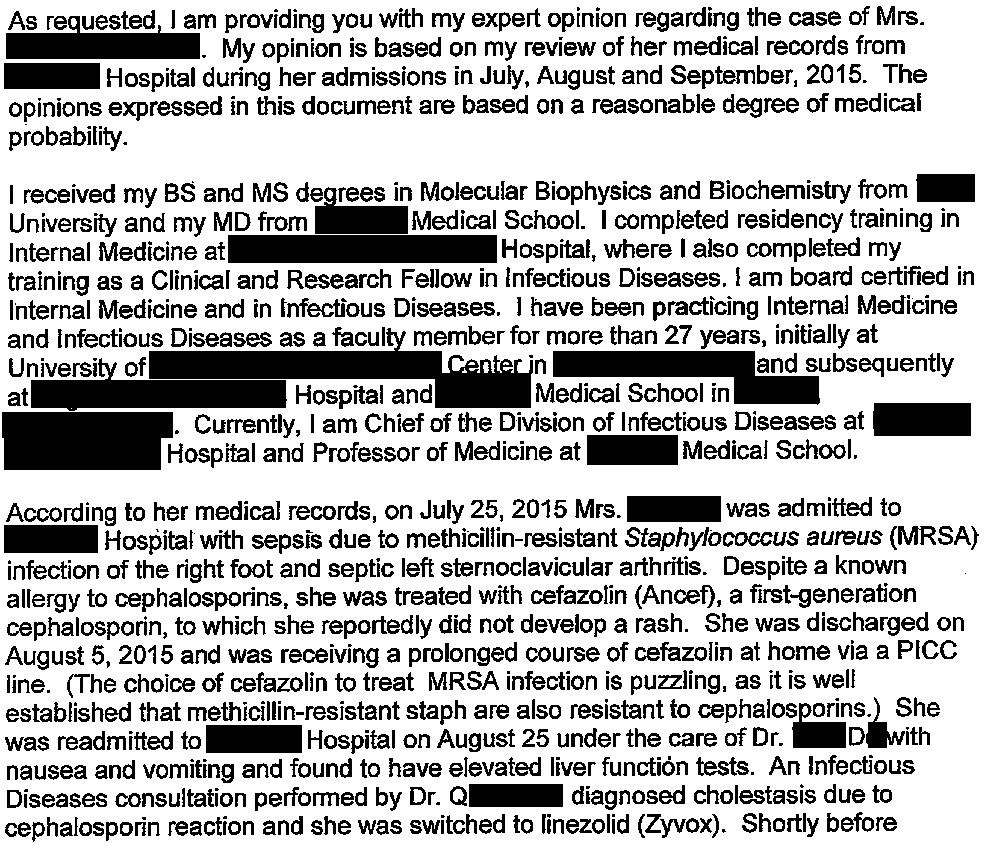
A 56-year-old woman was admitted with sepsis from a right foot infection.
She was later found to have septic arthritis of the left sternoclavicular joint.
The patient was started on cefazolin.
Cultures ultimately grew MRSA.
She was discharged after a month-long hospitalization, still on cefazolin.
Several weeks later, she developed nausea and vomiting.
She was readmitted, and noted to have elevated LFTs.
Dr. D was the admitting hospitalist, and Dr. Q was the consulting infectious disease specialist.
Dr. Q felt that the patient had developed cephalosprin-induced cholestatic drug-induced liver injury (DILI).
He recommended switching to linezolid.
The patient improved over about one week of hospitalization.
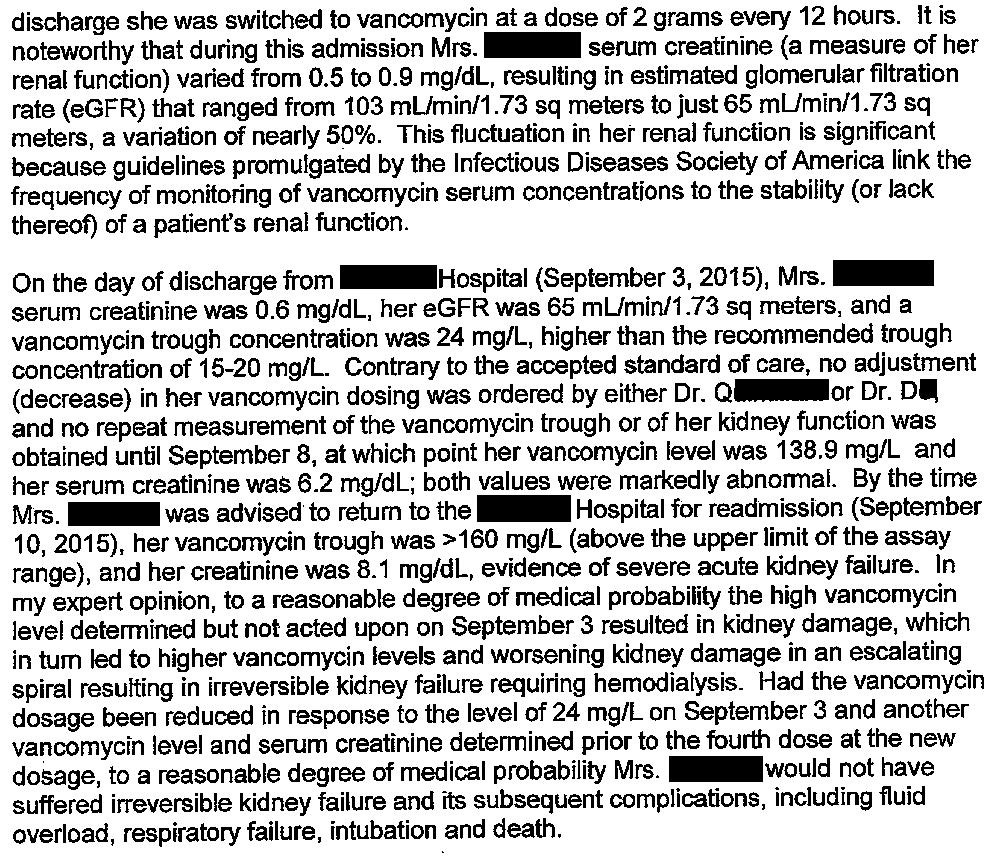
Near discharge, Dr. Q recommended switching to vancomycin.
Dr. D (hospitalist) ordered the vancomycin order set, which by default included trough levels.
He helped coordinate the patient’s discharge including PICC line, outpatient IV vancomycin orders, and rechecking levels a few days later.
5 days after discharge, repeat labs showed an extremely elevated vancomycin level and acute kidney injury with a creatinine of 6.2mg/dL.
She was readmitted to the hospital.
After initial improvement on dialysis, she declined and died in the hospital a month later.
We’re all prone to errors from time to time.
Avoid malpractice cases by proactively reviewing other doctors’ mistakes, rather than waiting for your own.
The patient’s husband hired a law firm.
They sued Dr. D (hospitalist), Dr. Q (infectious disease), their employers, and the hospital.
An infectious disease expert wrote the following opinion:
Each physician had their own defense attorney.
Dr. Q’s defense attorney hired an IM-trained hospitalist to blame Dr. D for the bad outcome.
Dr. Q’s attorney also hired a pharmacist to blame the hospital pharmacy for not contacting Dr. D.

Become a better doctor.
Paying subscribers get a new case every week and access to the archive.
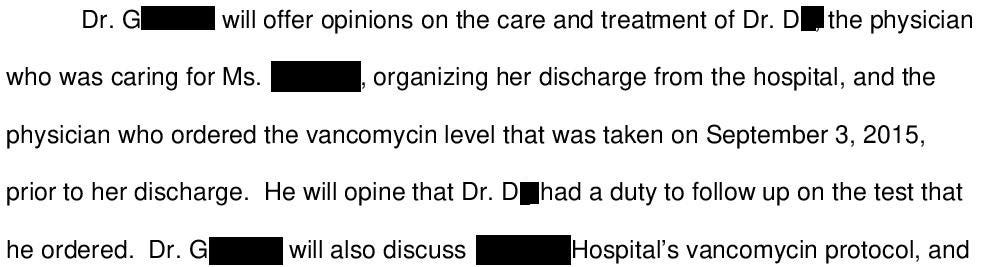
Dr. D’s defense attorney also disclosed 2 experts.
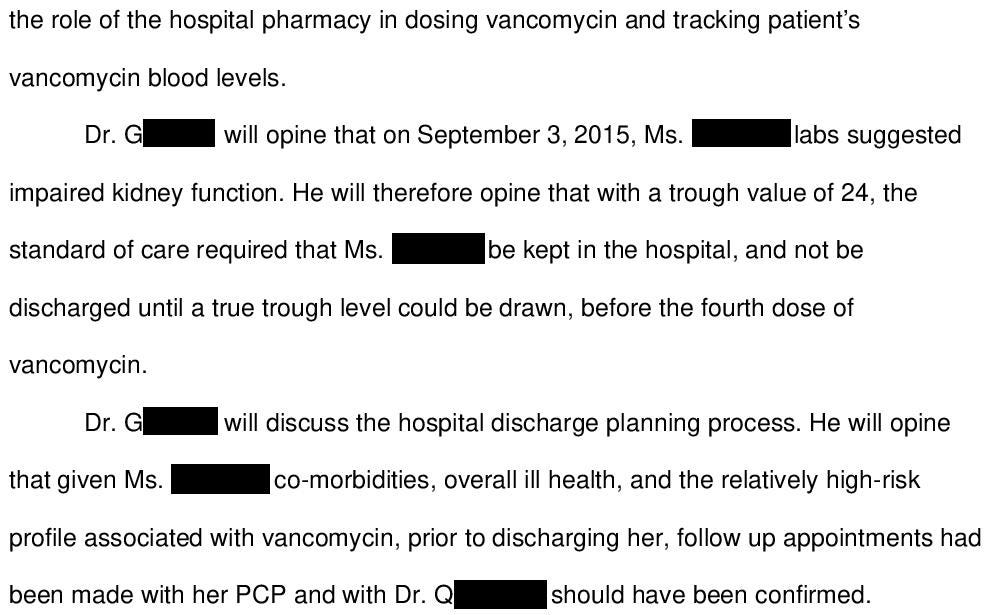
The first is an IM-trained hospitalist:
Dr. D’s second expert was a nephrologist who suggested that the patient’s death actually had nothing to do with her drug-induced kidney issues.
They suggest that she died as a result of TRALI after a blood transfusion.
The case reached a confidential settlement.
MedMalReviewer Analysis:
It’s quite odd that none of the doctors from the first hospitalization were sued. Discharging a patient with a confirmed MRSA infection on cefazolin is nonsensical and below the standard of care. I’m a bit baffled how she survived given it seems like she probably had MRSA bacteremia (presence of a septic sternoclavicular joint is strongly associated with bacteremia, up to 62% of the time in this review paper). The ultimate irony here is that it seems like she may have fought off MRSA bacteremia on her own (impressive and rare), then was killed by the downstream consequences of the correct treatment. It’s embarrassing to be part of a medical system that can fail patients so badly every step of the way. You’ve probably heard of the Swiss cheese model of errors… this case had more holes than it had actual cheese.
The ID specialist has a very good defense. It’s not his job to coordinate discharge planning or make sure the subsequent drug monitoring is done correctly, especially for a drug as common as vancomycin.
The biggest question in this case is how much blame the hospitalist should take. He was the one who placed the discharge order around the time she had an elevated vancomycin trough, which wasn’t even before the 4th dose. However, it seems like vancomycin dosing is often left to the pharmacists and runs on a fairly routine protocol without any input from the physician. Dr. D assumed it would be taken care of by the pharmacy, just like it had probably been done in every one of the other thousands of cases in his career that had been managed safely. He may have also felt significant administrative pressure to discharge patients as fast as possible, and felt that he wasn’t taking much risk with only a very mildly elevated result and thoughtful plan to recheck in a few days.
One of the hard parts about this case is seeing the hospitalist get attacked not only by the plaintiff’s attorney, but also by the ID physician’s attorney. Going through a malpractice case is very emotionally and psychologically challenging, which is only worsened when your own colleagues point out your errors. If this happens to you, it’s important to remember that this is routine legal strategy. Do your best to not let it affect you mentally or take it personally (easier said than done). You can proactively build resilience and steel yourself by understanding this tactic before you’re ever named in a lawsuit.
Here are some other related cases:
Case with very similar pattern involving monitoring of outpatient IV antibiotics (this one was about gentamicin instead of vancomycin).
Multiple (allegedly unnecessary) different antibiotics given to a patient who ultimately dies, possibly due to azithromycin/warfarin interaction.
A different drug-induced liver injury case (this one from valproate instead of cefazolin).
Criticism about hospital discharge planning related to anticoagulation (albeit somewhat unreasonable criticism).
Multiple (allegedly unnecessary) antibiotics given to patient with sinus discomfort, she ends up with severe neuropathy from levofloxacin.
DILI can cause kidney injury (kidney gets overwhelmed by prolonged liver toxicity). This goes back to the first hospitalization and that inappropriate and prolonged cefazolin use. Sometimes lawsuits focus myopically on timing rather than root cause. The 2nd hospitalization was consequent to the first one, yet only the 2nd got blamed.
“You’ve probably heard of the Swiss cheese model of errors… this case had more holes than it had actual cheese.” LOL. I’m going to have to adopt this turn of phrase, as it applies only too often in our current medical system.